Analytic Hierarchy Process for Prioritizing Radiation Safety Measures in Medical Institutions
Article information

Abstract
Background
This study aimed to prioritize policy measures to improve radiation safety management in medical institutions using the analytic hierarchy process.
Materials and Methods
It adopted three policy options—engineering, education, and enforcement—to categorize safety management measures, the so-called Harvey’s 3Es. Then, the radiation safety management measures obtained from the current system and other studies were organized into action plan categories. Using the derived model, this study surveyed 33 stakeholders of radiation safety management in medical institutions and analyzed the importance of each measure.
Results and Discussion
As a result, these stakeholders generally identified enforcement as the most important factor for improving the safety management system. The study also found that radiation safety officers and medical physicists perceived different measures as important, indicating clear differences in opinions among stakeholders, especially in improving quality assurance in radiation therapy. Hence, the process of coordination and consensus is likely to be critical in improving the radiation safety management system.
Conclusion
Stakeholders in the medical field consider enforcement as the most critical factor in improving their safety management systems. Specifically, the most crucial among the six specific action plans was the “reinforcement of the organization and workforce for safety management,” with a relative importance of 25.7%.
Introduction
In South Korea, the use of radiation is regulated by the Nuclear Safety Act, which is based on the recommendations of the International Commission on Radiological Protection (ICRP) 60. The act controls the use of radioisotopes and radiation generators (excluding those used for diagnostics) in patient diagnosis and treatment. As of June 2023, a total of 162 medical institutions in South Korea have been authorized to use radioisotopes or radiation generators. Since all citizens have access to medical institutions, ensuring the safe use and management of radiation is crucial. In addition, the International Atomic Energy Agency (IAEA) recommends that governments, regulatory authorities, and technical and scientific support organizations continue to search for technical and policy options to manage radiation safety [1]. Particularly, since the general public recognizes radioactive materials as dangerous substances, policy acceptance could be improved by making decisions based on scientific evidence, which requires both theoretical and empirical research to secure scientific data on radiological risks and consider the opinions of stakeholders from medical institutes.
Protection optimization is a fundamental principle in formulating radiation protection policies; it considers technical, economic, and social factors to establish the most effective protection system. Its goal is to minimize workers and the public’s radiation exposure to the lowest reasonably achievable level. In the beginning, this was accomplished through quantitative methods such as the cost–benefit analysis of protective options, which then developed from a more judgment-based approach to a decision-making process encompassing operational procedures, best practices, and qualitative considerations. According to the ICRP, the optimization principle entails the reduction of personal dose levels, the number of exposed individuals, and potential exposures to the lowest that is feasibly attainable under appropriate dose/risk constraints while considering economic and social factors [2], involving not only simple costs and primary benefits but also nonquantitative factors such as the psychological burden or social backlash due to radiation exposure. If many factors and alternatives exist, ensuring the objectivity of conclusions would be challenging. Therefore, an analytical method that can integrate both qualitative and quantitative indicators is required.
Radiation safety management aims to prevent harmful deterministic effects caused by radiation exposure on individuals and to limit stochastic effects to a permissible level. Accomplishing this goal requires the establishment of a radiation protection plan, such as the environmental monitoring of facilities, personnel exposure management, radiation safety education, and the implementation of safety equipment standards. Studies in medical institutions have sought to enhance radiation safety management by primarily proposing accident risk reduction through analyses of accident cases or expert investigations. While some studies have recognized policy-related issues, such as the need for continuous education to enhance expertise or the importance of fostering a safety culture within the organization, the majority of research endeavors have focused on disaster prevention methods related to technical (engineering) aspects, specifically shielding design and prevention strategies concerning the technical facets of radiation utilization [3–7]. However, in medical institutes, enhancing radiation safety management requires not only technical approaches but also educational and regulatory strategies, which need to be comprehensively integrated and quantitatively evaluated to determine implementation plans [8, 9].
Analytic hierarchy process (AHP) has been utilized as a decision-making methodology in various fields that require consideration of both quantitative and qualitative aspects. In the medical field, there has been a study to understand the importance of user requirements for computed tomography scanners using AHP [10]. Similarly, in the field of nuclear safety, AHP-based task analysis has been proposed to analyze multi-attribute tasks and decison making [11]. A study in the field of radiation safety management analyzed the relative importance of radiation worker safety management using the AHP from an integrated perspective, but it was limited by the absence of specific measures [12]. Since the characteristics and usage of radiation sources differ among the medical, industrial, and research fields, detailed approaches to establish radiation safety management plans in each field must be developed. In the present study, therefore, we aim to determine the relevance of specific implementation measures for improving radiation safety management in medical institutions using AHP, which is an effective tool for deriving the relative importance between various factors. This study could provide a foundation for future studies and policymaking on radiation safety management in medical institutions.
Materials and Methods
1. Overview of Research Methods
In Korea, the regulatory scope of the Nuclear Safety Act includes therapeutic radiation generators in radiation oncology and radioactive isotopes in nuclear medicine. The act incorporates the basic principles of radiation protection, justification, and optimization. It also considers persons undergoing medical procedures (diagnostic and therapeutic), pregnant women and their embryos/fetuses, infants of lactating patients, caregivers of patients, and volunteers in radiation-based biomedical research as subjects of medical radiation exposure management. In addition, it addresses issues associated with the mitigation of potential medical radiation exposure through informed consent, quality assurance to maintain patient exposure to radiation or administered radioactivity by medical prescriptions, and safety management for patients who are administered radioactive isotopes to minimize the unnecessary exposure of surrounding individuals and reduce environmental impact.
This study aims to quantitatively assess the importance of options for managing radiation safety in medical facilities, including engineering, education, and enforcement, and to provide objective evidence for system improvement and policy development prioritization. First, to derive specific strategies for improving radiation safety management in medical facilities, we organized the structure of the nuclear safety regulatory system and examined the national medical radiation safety regulatory system. Next, we identified and structured risk factors by analyzing administrative sanctions imposed on South Korean medical institutions (fines and penalties from 2012 to 2021, publicly available records) and case studies of incidents within the current regulatory framework. We then used these risk factors to formulate concrete approaches to mitigate them based on the literature and preliminary expert interviews. We developed a hierarchical model based on these proposed approaches and determined their relative importance through surveys of experts affiliated with medical institutions and relevant organizations, along with objective analytical methods.
2. Analytic Hierarchy Process
This study adopted AHP to assess the relative importance of policy measures and clarify the direction of policy options for improving radiation safety management in medical institutions in South Korea. AHP allows for the discovery of optimal options by stratifying evaluation criteria and deriving importance from multicriteria decision-making problems involving several decision makers [13]. The process is as follows:
(1) Define the decision-making problem. Examples include barriers to the implementation of medical waste management [14], obstacles to renewable energy development [15], and factors of nuclear power plant design [16].
(2) Structure a decision hierarchy based on decision-making factors, which are typically derived from literature reviews. Decision hierarchies constructed by researchers are sometimes reviewed by experts using surveys.
(3) Create pairwise comparison questions for each decision hierarchy level. These questions are structured so that all pairwise comparisons can be made between factors in the level. If the level consists of n factors, the number of pairwise comparison questions should be n(n−1)/2 [17]. Table 1 shows an example of a pairwise comparison question. A nine-point Likert scale is commonly used for comparisons between factors, in which 1 point is assigned when the importance of two factors is the same and 2–9 points are assigned to each side. For example, if a respondent assigns 3 points on the right side, then that respondent considers the factor on the right to be three times as important as the one on the left.
(4) Organize survey respondents using appropriate sampling methods that can help administer the survey and achieve its purpose. This involves defining the population and ensuring that the respondents are representative of it. For example, when a researcher investigates the priority of energy policy measures, the population can include groups engaged in energy policy decison making processes (e.g., policymakers, researchers, business expert groups, etc.). In this case, the sample should be determined by considering the influence and size of the group so that they represent the population. One way to do this is to organize respondents in proportion to their weight within the population.
-
(5) After gathering the participants’ responses, estimate the vector of relative weights on factors affecting decison making using the eigenvalue method. Pairwise comparison matrix A is defined as Equation (1), where aij indicates a comparison result between factors i and j. For example, if a respondent stated that factor i is twice as important as factor j, aij and aji should be 2 and
(1) -
(6) Matrix w is the relative importance matrix corresponding to the maximum eigenvalue λmax among the n eigenvalues λ1, λ2, …, λn which satisfy Equation (2), where ∑λi=n. If a respondent has perfect consistency, λmax equals n.
(2) -
(7) Evaluate the consistency of a participant’s responses based on the estimated maximum eigenvalue λmax. This is conducted using the consistency index (CI) in Equation (3) and the consistency ratio (CR) in Equation (4). Here, the random consistency index (RCI) indicates the CI for a randomly generated pairwise comparison matrix A. If the CR for a respondent is less than 0.2 (20%), the result of the respondents’ pairwise comparison is considered consistent; otherwise, their results are excluded from analysis.
(3)(4) (8) Aggregate the relative importance matrices of respondents that show consistency. To obtain comprehensive results, this study used the arithmetic average of the relative importance of individual respondents.
3. AHP Hierarchy Construction
Although technological advances in medical radiation have significantly reduced unnecessary patient exposure, their increased complexity has also introduced new forms of human error and equipment issues. A study that analyzed 10 years of participation in the IAEA Quality Assurance Team for Radiation Oncology program in the European region identified vital factors that compromised the quality of radiation therapy, which include insufficient staffing, education/training, equipment, and quality management [18]. Hence, improving radiation safety management in medical institutions necessitates a comprehensive analysis of technical, human, and systemic inadequacies.
In this study, we established an AHP model based on Harvey’s 3E framework as a means to enhance radiation safety management systems (Table 2). For subcategories, we obtained specific sub-items by reviewing radiation safety regulations, administrative sanctions and case studies, and research findings [3–9]. Additionally, in the case of the radiation therapy field, we explored measures to address factors that contribute to radiation accidents according to ICRP 86, such as inadequate education and training, a lack of quality assurance, inadequate infrastructure, equipment malfunctions, and inappropriate decommissioning [19]. In nuclear medicine, in accordance with ICRP 140 recommendations, we explored measures to optimize radiation protection and reduce external radiation exposure and contamination, maintain low radiation background levels to prevent interference with imaging devices, ensure proper waste isolation, and enhance personnel safety and security (entry and exit control) [20].

Details of Categories (Level 2) in the Analytic Hierarchy Process Model
The highest level of the hierarchy (level 1) corresponds to the ultimate goal of the decision-making process, while the lower levels consist of factors that influence decisions at the higher levels. As the hierarchy progresses downward, more specific implementation strategies are identified to achieve the overall goal. This study proposes the following implementation strategies within the hierarchical model: (1) minimizing medical radiation exposure risks due to accidents; (2) maintaining patients’ exposure to radiation or administered radioactivity in accordance with medical prescriptions through quality assurance; and (3) managing the safety of patients administered with radioactive isotopes to reduce unnecessary exposure of surrounding individuals and the potential environmental impact. As shown in Fig. 1, these strategies were organized in a specific hierarchical structure.

Hierarchy structure of the analytic hierarchy process model.
4. Survey Description
Pairwise comparison questions were formulated for each decision hierarchy level, as shown in Table 1. The survey respondents were 33 radiation safety management experts in South Korean medical institutions. To consider the opinions of various stakeholders, this study recruited radiation safety officers, medical physicists, and regulators. The survey was conducted online between October and November 2022. Table 3 presents the characteristics of the survey respondents.
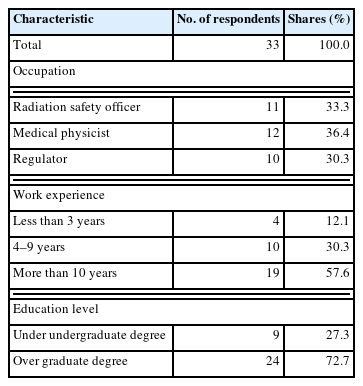
Characteristics of Survey Respondents
Results and Discussion
1. Data Description
Of the 33 total respondents, the pairwise comparison results of those who showed consistency were used in the analysis. As mentioned above, pairwise comparison results were considered consistent when the CR was less than 0.2 based on the literature. Accordingly, the analysis included the pairwise comparison results of 19 of the 33 respondents. The number of respondents in each stakeholder group was determined based on the population distribution of medical physicists and radiation safety officers, resulting in similar numbers in both groups. Furthermore, the number of respondents in the regulator group was also selected to be similar to that of the other groups to prevent bias against any particular group. Table 4 summarizes the number of samples with CRs of 0.2 or less for each respondent group.

Number of Respondents with CR ≤0.2
2. Results: Total Respondents
As shown in Fig. 2, the respondents considered enforcement (42.3%) the most important category of policy options for improving radiation safety management in medical institutions (level 2), followed by engineering (33.4%) and education (24.3%). In other words, stakeholders in medical radiation who participated in this survey believe that the most important factor for the improvement of radiation safety management in medical institutions is the emphasis on policy options related to regulations. Meanwhile, the respondents placed little importance on education that focuses on the development of their capabilities.

Relative importance of policy measure categories (level 2).
Next, the relative importance of action plans (level 3) is shown in Fig. 3. The relative importance of a certain action plan among all plans is calculated by multiplying the relative importance of the category (level 2) to which the plan belongs by that of the plan among those within the same option. For example, the relative importance of “improvement of quality assurance in radiation therapy (Eng1)” among the six action plans is derived as 15.6% by multiplying 33.4% (the relative importance of “engineering” in level 2) by 39.3% (the relative importance of “Eng 1” within the “engineering” category).
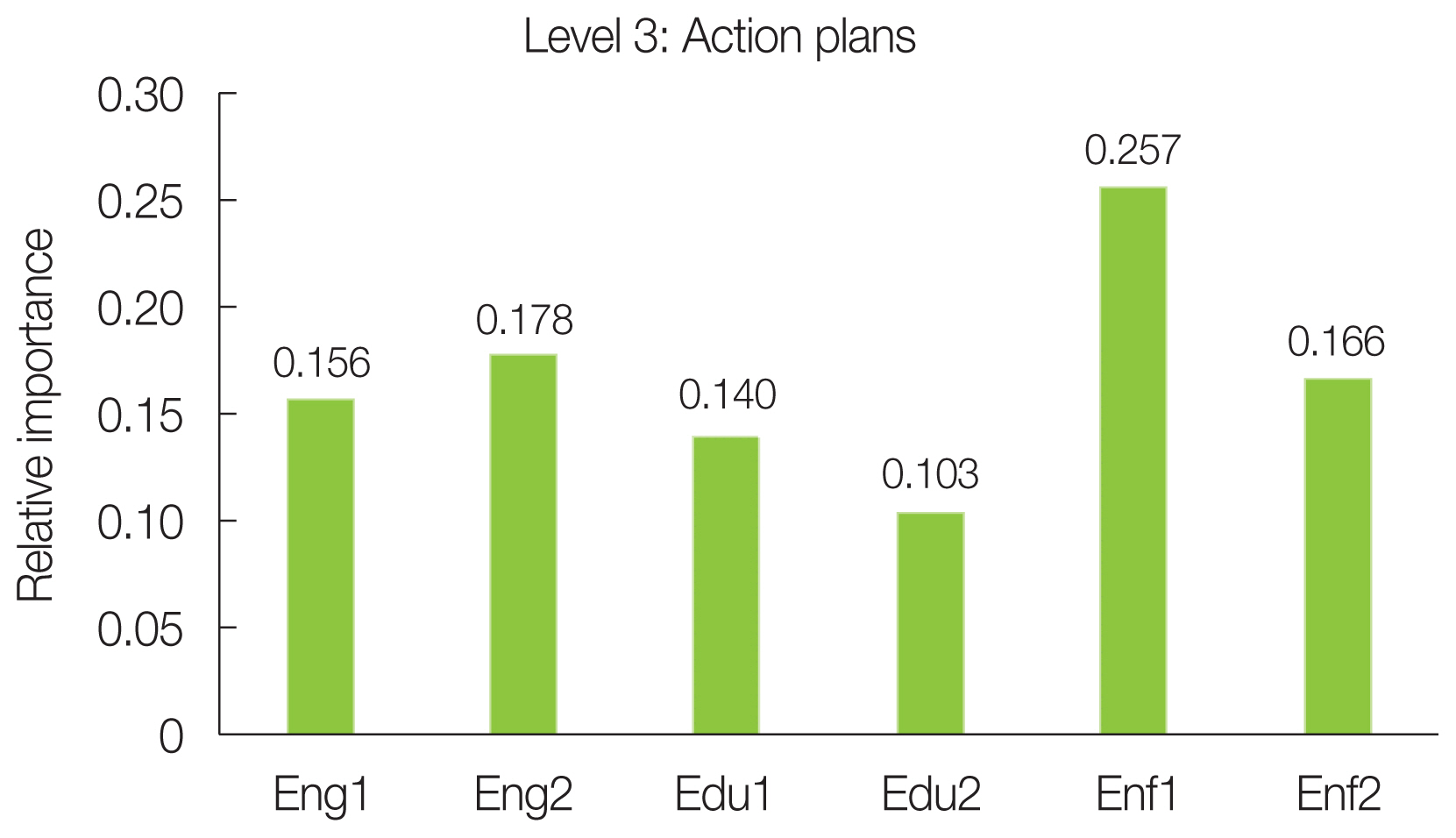
Relative importance of action plans (level 3). Improvement of quality assurance in radiation therapy (Eng1), segmentation of safety management equipment/facility standard (Eng2), reinforcement of radiation safety officers training (Edu1), strengthening regulator expertise (Edu2), reinforcement of organization/workforce for safety management (Enf1), improvement of management system for the regulated (Enf2).
Fig. 4 facilitates the comparison of the relative importance between action plans. The respondents considered “reinforcement of organization/workforce for safety management” the most important action plan (25.7%) for the enhancement of radiation safety management in medical institutions. Simply put, the general opinion of the participants in the medical radiation stakeholder group highlights the need to reinforce the current organization and workforce for safer radiation management in medical institutions. Next, “segmentation of safety management equipment/facility standard” (17.8%), “improvement of management system for the regulated” (16.6%), and “improvement of quality assurance in radiation therapy” (15.6%), in that order, were found to be important. However, the respondents generally did not assign a relatively high importance to education-related action plans such as “reinforcement of radiation safety officers training” (14.0%) and “strengthening regulator expertise” (10.3%).

Priority of improving radiation safety management (presented in hierarchy). The italics (gray) indicate the relative importance within each level (local relative importance), and the normal font (black) indicates the overall relative importance in the final hierarchy (global relative importance).
3. Results: by Respondent Group
The respondents’ opinions on radiation safety management were analyzed and compared by stakeholder group (Fig. 5). Table 5 summarizes the differences in respondent groups’ perceptions of the importance of factors in level 2.

Radial plot of relative importance: (A) level 2 and (B) level 3.
Relative Importance of Policy Options (Level 2) by Stakeholder Group
Each group clearly had different policy measure categories that they considered important. The radiation safety officers and regulators shared the perception that “enforcement” is the most vital option in level 2, while medical physicists considered “engineering” the most critical. In addition, regulators placed relatively similar importance on three policy options, but radiation safety officers and regulators assigned significantly greater importance on others.
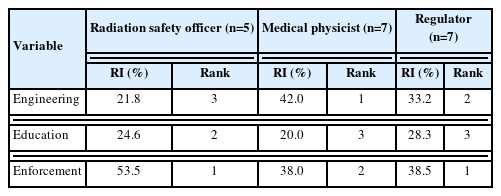
Table 6 presents the relative importance on action plans (level 3) by group. The action plans with the highest priority were “reinforcement of organization/workforce for safety management” (41.6%) for radiation safety officers, “improvement of radiation therapy quality assurance” (26.9%) for medical physicists, and “reinforcement of organization/workforce for safety management” (22.4%) for regulators. Notably, radiation officers and regulators evaluated “improvement of quality assurance in radiation therapy,” which medical physicists regarded as the most important, as the action plan with the lowest priority. This means that only medical physicists are aware of the significance of improving radiation therapy quality assurance for safer management of radiation in medical institutions. “Reinforcement of organization/workforce for safety management” was evaluated as the most important plan by radiation safety officers and regulators and was also recognized by medical physicists as the third most important plan. This highlights the need to prioritize strengthening the organization/workforce to improve the safety management of radiation in medical institutions in South Korea.

Relative Importance of Action Plans (Level 3) by Stakeholder Group
Another notable finding is that radiation safety officers and medical physicists, who belong to the regulated group, placed relatively low importance on “strengthening regulator expertise” (6.9% and 8.1%, respectively), while regulators rated it as somewhat important (15.0%). This suggests that regulators themselves are aware that they must improve their expertise and capability.
Conclusion
Because medical facilities are open to the public and present various risks, it is necessary to integrate all engineering, educational, and enforcement options to assess them quantitatively and devise action plans to construct a radiation safety management system. However, studies have mainly focused on engineering aspects when examining shielding design and preventive measures. Hence, this study aimed to improve radiation safety management by developing specific policy measures that include technical, educational, and regulatory elements and evaluate these options using AHP to determine the relative importance of each implementation approach. The findings could provide a basis for the development of radiation safety management policies. Furthermore, decison making based on scientific evidence could help derive reasonable regulatory directions and improve policy acceptance.
The current results can be summarized as follows. First, stakeholders in the medical field view enforcement as the most important factor for improving their safety management systems. The most crucial among the six specific action plans was the “reinforcement of the organization and workforce for safety management,” with a relative importance of 25.7%. Second, although each category is equally significant for regulators, there are remarkable differences in the assigned importance perceived by radiation safety managers and medical physicists. For medical physicists, the most critical measure is the enhancement of quality assurance in radiation therapy, while radiation safety managers consider it a less significant implementation strategy. Rather, radiation safety managers rated the reinforcement of organization/workforce for safety management as critical. This finding is likely due to the two groups’ different perceptions of current problems with radiation safety management in medical institutions. According to the results of the survey on perceived problems with current safety management, radiation safety managers identified a shortage of safety managers as the biggest problem with current radiation safety management. On the other hand, medical physicists perceived a lack of communication between regulators and regulated groups and a lack of governance of radiotherapy quality management as the biggest problems in current radiation safety management. Third, in the case of enhancing regulatory expertise, radiation safety managers and medical physicists, who are regulated groups, consider its significance to be relatively low, while regulators themselves evaluate it as somewhat more important.
From the results, certain policy measures can be derived. Overall, stakeholders regard “reinforcement of the organization and workforce for safety management” as the most urgent measure to enhance radiation safety management in the medical field. In addition, differences in opinions between radiation safety managers and medical physicists emphasize the importance of coordination and consensus among them. This process is crucial for enhancing radiation safety management systems as the lack of adequate consensus may hinder policy implementation. Finally, further analysis must fully understand the disparity in regulatory expertise perception between regulators and regulated groups and consider various possibilities, including scenarios where a higher level of regulatory expertise is likely to result in greater regulatory strength.
The limitations of this study and recommendations for future research are as follows. First, this study excluded the viewpoints of physicians, nurses, radiologists, and other professionals; thus, the results may not entirely reflect the viewpoints of all medical stakeholders. Second, the analysis was limited to the average perception of opinions within groups. Since opinions within groups may vary, the multidimensional aspects of the opinions of each stakeholder group must be examined. For example, regulators seem to have assigned comparable importance at level 2. Research must determine whether this is because regulators follow a general trend of placing similar importance on all three options or because opinions are distributed across the extremes, resulting in similarity that has been averaged out. Overcoming these limitations in future research will lead to a better understanding of radiation safety management, yielding more detailed insights for policy and practice.
Notes
Conflict of Interest
No potential conflict of interest relevant to this article was reported.
Ethical Statement
According to Bioethics and Safety Act in Republic of Korea, neither approval from the ethics committee nor informed consent from the study populations is required for this study.
Author Contribution
Conceptualization: Kim HS, Moon H. Data curation: Kim HS, Moon H. Formal analysis: Kim HS, Moon H. Funding acquisition: Moon H, Park SH. Methodology: Kim HS, Moon H. Project administration: Kim HS, Park SH. Visualization: Kim HS, Jeong H, Moon H. Writing - original draft: Kim HS, Jeong H, Moon H. Writing - review & editing: Park SH. Approval of final manuscript: all authors.
Acknowledgements
This work was supported partially by the National Research Foundation of Korea (NRF) grant funded by the Korea government (MSIT) (Project No.: 2022R1F1A1076189, RS-2023-00242528), and partially by the Korea Institute of Nuclear Safety (Grant No. S2361169).

