Detection Limit of a NaI(Tl) Survey Meter to Measure 131I Accumulation in Thyroid Glands of Children after a Nuclear Power Plant Accident
Article information

Abstract
Background
This study examined the detection limit of thyroid screening monitoring conducted at the time of the Fukushima Daiichi Nuclear Power Plant (FDNPP) accident in 2011 using a Monte Carlo simulation.
Materials and Methods
We calculated the detection limit of a NaI(Tl) survey meter to measure 131I accumulation in the thyroid gland of children. Mathematical phantoms of 1- and 5-year-old children were developed in the simulation of the Particle and Heavy Ion Transport code System code. Contamination of the body surface with eight radionuclides found after the FDNPP accident was assumed to have been deposited on the neck and shoulder area.
Results and Discussion
The detection limit was calculated as a function of ambient dose rate. In the case of 40 Bq/cm2 contamination on the body surface of the neck, the present simulations showed that residual thyroid radioactivity corresponding to thyroid dose of 100 mSv can be detected within 21 days after intake at the ambient dose rate of 0.2 μSv/hr and within 11 days in the case of 2.0 μSv/hr. When a time constant of 10 seconds was used at the dose rate of 0.2 μSv/hr, the estimated survey meter output error was 5%. Evaluation of the effect of individual differences in the location of the thyroid gland confirmed that the measured value would decrease by approximately 6% for a height difference of ±1 cm and increase by approximately 65% for a depth of 1 cm.
Conclusion
In the event of a nuclear disaster, simple measurements carried out using a NaI(Tl) scintillation survey meter remain effective for assessing 131I intake. However, it should be noted that the presence of short-half-life radioactive materials on the body surface affects the detection limit.
Introduction
The tsunami caused by the Great East Japan Earthquake of March 11, 2011 spread across eastern Japan and caused extensive damage to the Fukushima Daiichi Nuclear Power Plant (FDNPP), which resulted in the release of radioactive materials into the atmosphere. Post-accident investigations revealed that the released radioactive materials included 134Cs, 137Cs, and 131I. The United Nations Scientific Committee on the Effects of Atomic Radiation report concluded that the total amount of 131I released into the environment ranges from about 100 to 500 PBq and the total amount of 137Cs is generally in the range of 6 to 20 PBq [1].
A similar large-scale nuclear accident occurred in 1986 at the Chernobyl nuclear power plant in the former Union of Soviet Socialist Republics. Post-accident studies showed that inhalation of 131I released into the atmosphere caused a significant increase in childhood thyroid cancers. The lessons learned from the Chernobyl and FDNPP accidents led to an emphasis on the importance of pediatric thyroid monitoring in the event of a large nuclear accident [2, 3].
Simple measurements using a NaI(Tl) scintillation survey meter are considered useful for emergency thyroid monitoring. Following the FDNPP accident, approximately 1,000 children were surveyed using these meters [4, 5]. However, their accuracy has been challenged because of simple measurements. In particular, both radioactive contamination of the body surface and the ambient dose rate from the surrounding environment can affect the detection of radioiodine [6, 7].
Radioactive materials released into the atmosphere are carried by wind and fall to the ground [8–10]. As a result, radioactive materials can adhere to the neck, shoulders, and other body surfaces of evacuees from the affected area around a nuclear accident. Studies have also been conducted for estimating the absorbed doses to thyroids based on body surface contamination levels [11–13]. Simple measurements are made by placing the detector in front of the neck and measuring the dose from the thyroid gland. The contributions from radioactive materials adhering to the neck, chest, and jaw can affect these measurements [4]. The contribution of radiation from the surrounding environment should also not be ignored. Normally, the ambient dose rate from the natural environment is approximately 0.05 μSv/hr [14]. However, a large amount of radioactive materials during the FDNPP accident was released into the environment, and the ambient dose rate exceeded several μSv/hr in some areas [1].
In simple measurements using a survey meter, the dose rate is displayed as a differential amount and constantly fluctuates because it measures randomly generated radiation. A reading error occurs when the measurer reads the counts on the digital display. This error represents the uncertainty associated with measuring radiation from the trace amounts of radioactive materials in the thyroid gland. As described above, uncertainty in the measured values cannot be avoided with simple measurements using NaI(Tl) survey meters. In July 2021 Nuclear Regulatory Commission reported on the development of a new detector suitable for thyroid screening [15]. The new detector has a probe structure tailored to the size of a child’s neck, and also can provide a good value of minimum detectable activity due to better energy resolution [16]. Nevertheless, it should be considered to use NaI(Tl) survey meters for easily measuring a large number of children in emergencies since the survey meters have been widely used for another purpose.
This study simulated radioactive contamination on the body surfaces of victims exposed to a radioactive plume and investigated the effect of this contamination on detection limits. The detection limits were evaluated taking into account the influence of ambient dose rate and reading errors in the survey meter output. Multiple short-half-life radioactive materials are released into the atmosphere during a nuclear power plant accident. The effects of short-lived nuclides other than 131I on the detection limits were also investigated.
Materials and Methods
Monte Carlo simulations employing the Particle and Heavy Ion Transport code System (PHITS) code were performed using a mathematical phantom. As 131I accumulation in the thyroid gland gives a higher dose at younger ages, 1- and 5-year-old children were targeted for analysis. The mathematical phantoms of 1- and 5-year-old children were created as shown in Fig. 1. This study used a stylized/mathematical phantom that approximates the body shape and neck/shoulder size of Japanese children, as shown in Fig. 1. Assuming the thyroid gland to be U-shaped, simulation was conducted; point sources were placed at five locations: right lobe (two locations), left lobe (two locations), and isthmus (one location) to reproduce the shape of the thyroid gland in the simulation. The depths of the thyroid gland in 1- and 5-year-old children were set with reference to the International Commission on Radiological Protection (ICRP) pediatric voxel phantoms. The right and left lobes of the thyroid gland were located slightly anterior to the center of the trachea, with the anterior surface of the thyroid gland at a depth of 2 cm below the neck surface and the posterior surface at a depth of 3 cm. Since the size and depth of the thyroid gland vary greatly in children under 5 years of age due to differences in growth rate, we set here 1-year-old children: 1.0 to 1.5 cm in length and width; 5-year-old children: 1.5 to 2.0 cm in length and width, and 1 cm in thickness for both. The depth of the thyroid gland was set at 2 cm from the surface of the neck to the anterior thyroid gland and 3 cm to the back of the thyroid gland. For children under 5 years of age, there are individual differences in the speed at which they grow. There are few papers that have reported the individual differences in the thyroid glands. Since a deeper depth has a greater impact on the survey meter’s reading, a depth of 3 cm was selected to avoid underestimation. The effects of the radiation source position from a depth of 3 cm (back of the thyroid gland) to a depth of 2 cm (front of the thyroid gland) on the measured values were simulated. The reason for setting the thyroid depth at the same place for 1- and 5-year-old children was that the thyroid size, neck size, and neck length varied by age, resulting in the same depth. The size of the thyroid gland was assumed to be 1.0 to 1.5 cm in length and width for 1-year-old children and 1.5 to 2.0 cm in length and width for 5-year-old children. The larger size of the thyroid gland would result in less radiation entering the survey meter than the smaller size. For this reason, the simulation was performed by setting the survey meter to a larger size that can bring a higher impact on the measured value of the survey meter.
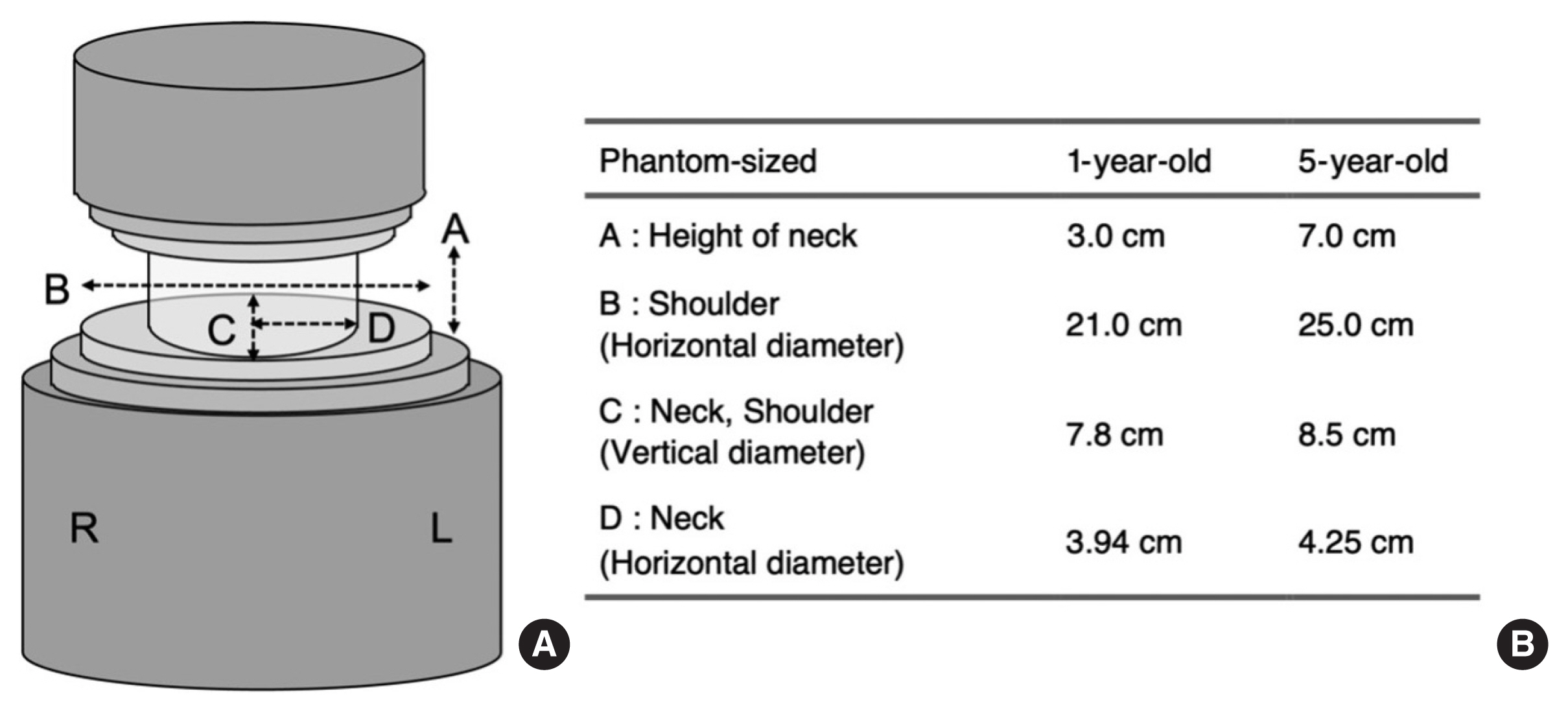
A mathematical phantom used for each age (A). The phantoms were developed for children aged 1 and 5 to conform to the Japanese body shape, and the neck and shoulder sizes are listed in the table (B).
For simple measurements, the NaI(Tl) scintillation detector probe was placed close to the neck. To reproduce the simple measurement in the PHITS code, the detector probe portion was set to the actual probe size of 2.5-cm-diameter with 2.5-cm-length, and the composition of Na and I was set to 1:1. Because the NaI scintillator is tidal, it was covered with 0.6 mm of aluminum on the inside and 1.5 mm of aluminum on the outside (Fig. 2). The detector probe was set at the center of the neck, at the level of the thyroid gland.
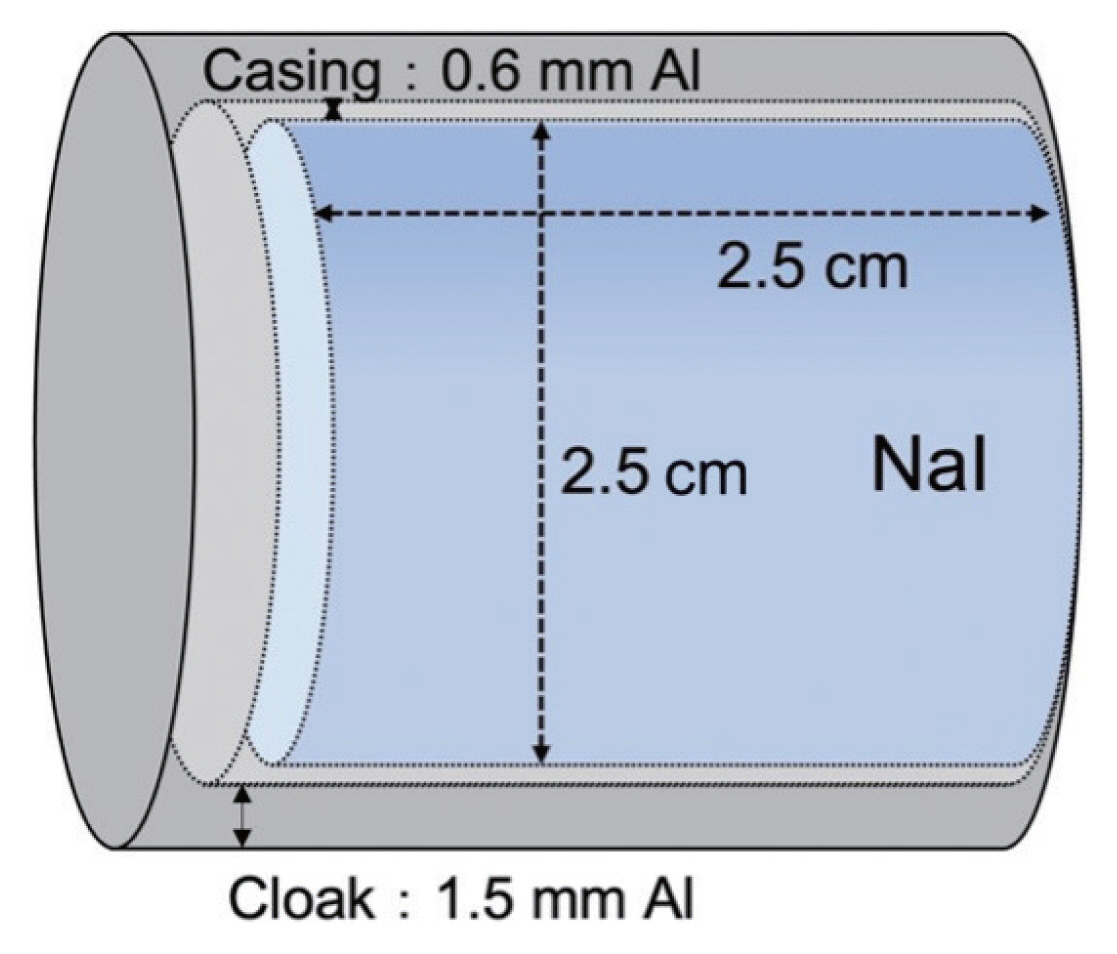
Probe geometry of a NaI(Tl) scintillation survey meter used in the Particle and Heavy Ion Transport code System simulation. The probe size was matched to that of the type of NaI(Tl) scintillation survey meter (TCS-161) used during the Fukushima Daiichi Nuclear Power Plant accident (NaI 2.5-cm-diameter with 2.5-cm-length, NaI casing 0.6 mm Al, cloak 1.5 mm Al).
The NaI(Tl) scintillation detectors commercially available and widely used in Japan display measured values as the 1 cm dose equivalent rate after the radiation energy correction. The PHITS code cannot directly determine the 1 cm dose equivalent rate. In order to treat it as a 1 cm dose equivalent rate value, the absorbed dose rate in the detector area obtained using the PHITS code must be converted to a 1 cm dose equivalent rate. Therefore, a conversion factor is needed to treat the absorbed dose rate calculated using the PHITS code as the 1 cm dose equivalent rate. The conversion coefficients were obtained such that the absorbed dose rate indicated by the NaI(Tl) scintillation survey meter probe located 1 m away from the source can be treated as the 1 cm dose equivalent rate (Table 1).
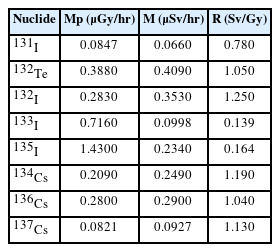
Conversion Factors Used for Simulating a NaI(Tl) Scintillation Survey Meter with an Energy-Compensating Type
Although eight radionuclides, 131I, 132I, 132Te, 133I, 135I, 134Cs, 136Cs, and 137Cs, were considered as a result of the accident at FDNPP, we mainly targeted 131I for estimating thyroid doses. The radiation field was set up such that each nuclide (1 MBq of radioactivity) was located 1 m away from the probe position. The absorbed dose rate in the probe region was obtained for each nuclide and compared with the 1 cm dose equivalent rate. The value obtained by the following equations was treated as the conversion factor.
Where R is conversion factor (Sv/Gy); M, 1 cm dose equivalent rate (μSv/hr); A, radioactivity (Bq); ΓH, 1 cm dose equivalent rate constant (μSv·m2·MBq−1·h−1) [17]; Mp, absorbed dose rate at the probe calculated using the PHITS code (μGy/hr); r, distance from source (m).
For the eight nuclides of contamination on the body surfaces of evacuees, we referred to the records obtained by measuring evacuees’ clothing using Geiger-Müller (GM) survey meters (Hitachi-Aloka Medical Ltd.) and two Ge γ-spectrometers (AccuScan; CANBERRA Industries Inc.) in the Fukushima Medical University Hospital on March 12 to 13 after the FDNPP accident [12]. With the back of the neck at 0°, the area of contamination was extended to the front of the neck in 18° increments centered on the center of the neck (Fig. 3A), assuming that children would be held by their guardians during evacuation. A total of 10,000 points were randomly set within the area determined by each angle, and the sources were placed at those locations. Contamination of the shoulder area assumed that radioactive materials were deposited directly above during the evacuation, leading to the deposition of radioactive materials over the entire shoulder area (Fig. 3B).
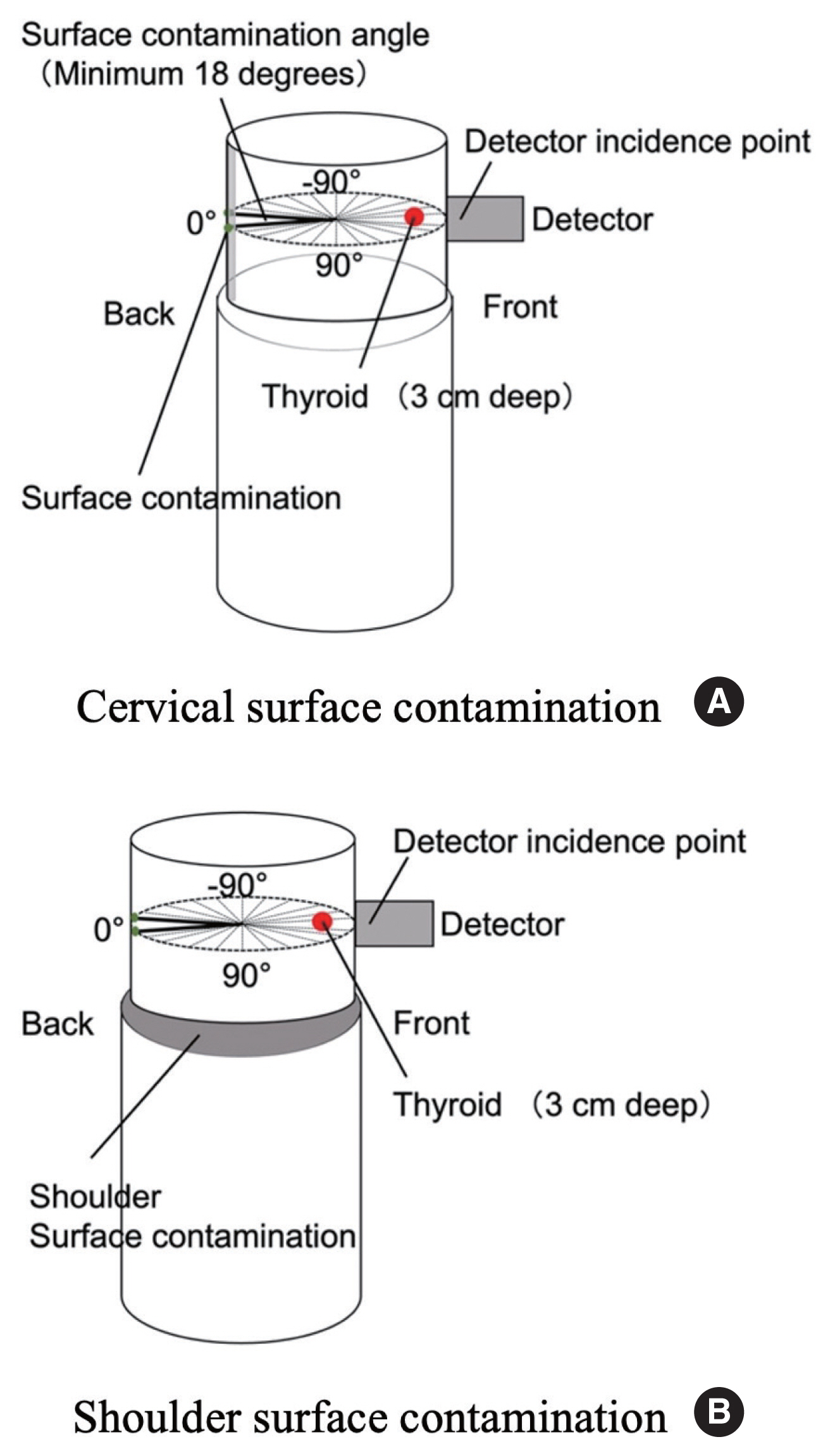
Extent of the body surface contamination by radioactive materials. Contamination of the body surface of the cervical region was extended in 18° increments from 0° at the back of the neck to the front of the neck (180°), with the center of the neck defined as the center. Shoulder contamination assumed a situation in which contamination spread uniformly over the entire collar opening: (A) extent of neck contamination, (B) extent of shoulder contamination.
The body surface contamination was 40 Bq/cm2, which was used as a screening reference for the body surface contamination during the FDNPP accident. A 40 Bq/cm2 contamination on the body surface corresponds to the thyroidal equivalent dose of 100 mSv [18]. This represents the expected density of contamination adhering to the body surface when an infant is exposed to air with a radioactivity concentration leading to 100 mSv for the thyroid gland when inhaling 131I. A dose of 100 mSv was treated by the Nuclear Safety Commission (now the Nuclear Regulatory Commission) as a reference thyroid dose for detailed pediatric thyroid examinations at the FDNPP accident [2].
Body surface contamination survey is performed using a GM survey meter. As a GM survey meter cannot identify nuclides, we assumed both an exposure scenario in which the body surface was contaminated with 40 Bq/cm2 of 131I and a scenario in which the body surface was contaminated with all eight nuclides.
The detection limit was obtained by dividing the 3σ (99.7% confidence level) value of the sum of the total 1 cm dose equivalent rates from contamination of the body surface and the ambient dose equivalent rate (0.2 μSv/hr) by the 1 cm dose equivalent rate of the thyroid gland per 1 Bq. The ambient dose rate in the measurement environment was set to 0.2, 1.0, and 2.0 μSv/hr. The value of 0.2 μSv/hr refers to the fact that when evacuees were measured at the FDNPP accident, the measurements were conducted at an ambient dose rate of 0.2 μSv/hr or less.
Here, the dose rate refers to the 1 cm dose equivalent rate, which is the value indicated by the survey meter. σ represents the standard deviation.
Results and Discussion
1. Survey Meter Reading Errors
The measurement error of the reading record by a survey meter was examined by varying the magnitude of the dose rate and the time constant of the survey meter. Random variation in output was experimentally obtained using 137Cs source. The time constant was varied from 3 to 30 seconds every 600 seconds for 1,800 seconds. Fig. 4 shows the change in the value of the digital multimeter connected to the output of the survey meter, and also shows the variation in output at ambient dose rates of 0.2 to 0.3 μSv/hr.
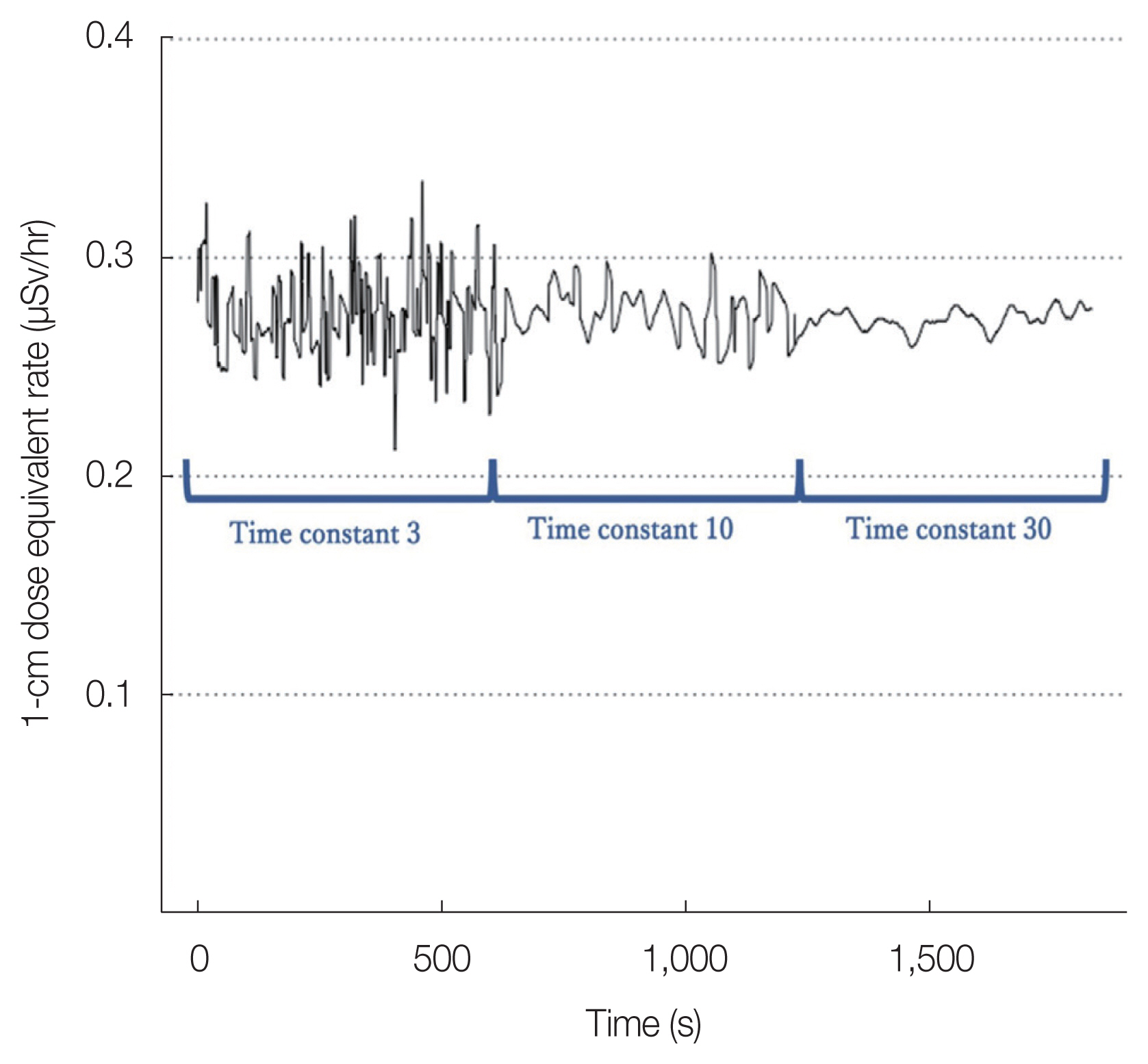
Output waveform when a digital multimeter is connected to the output terminal of the NaI(Tl) scintillation survey meter. The output waveform (displayed value) when the time constant is changed to 3, 10, and 30 seconds at 10 seconds intervals. The output waveform depends on the dose rate, and Fig. 8 shows the variation when the dose rate is approximately 0.3 μSv/hr.
Variation is expressed as the relative standard deviation and measured as a function of dose rate and time constant, as shown in Fig. 5. The greatest variation in output was observed when both the dose rate and time constant were low. It can be seen that an error of 5% to 10% was unavoidable at ambient dose rates of 0.2 μSv/hr or lower. This variation was equivalent to the actual measured doses of 0.01 to 0.07 μSv/hr recorded as measured doses from the thyroid gland in Fukushima [19].
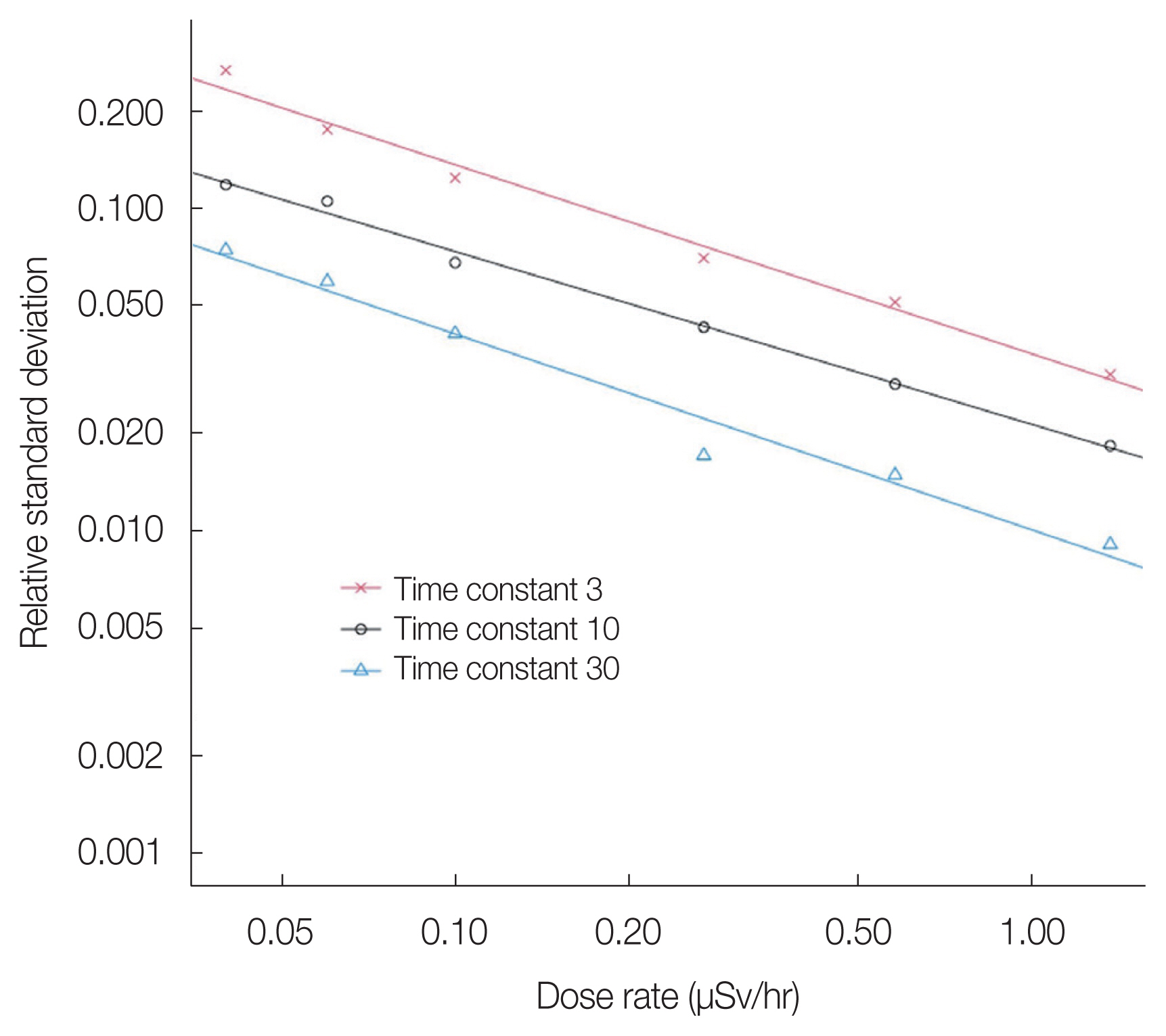
Comparison of the degree of output variation appearing in the output waveforms when the time constant and dose rate were varied, in terms of relative standard deviation. The figure shows that the smaller the time constant and the lower the dose rate were, the larger was the relative standard deviation.
2. 1 cm Dose Equivalent Rate from Contamination of the Cervical Body Surface
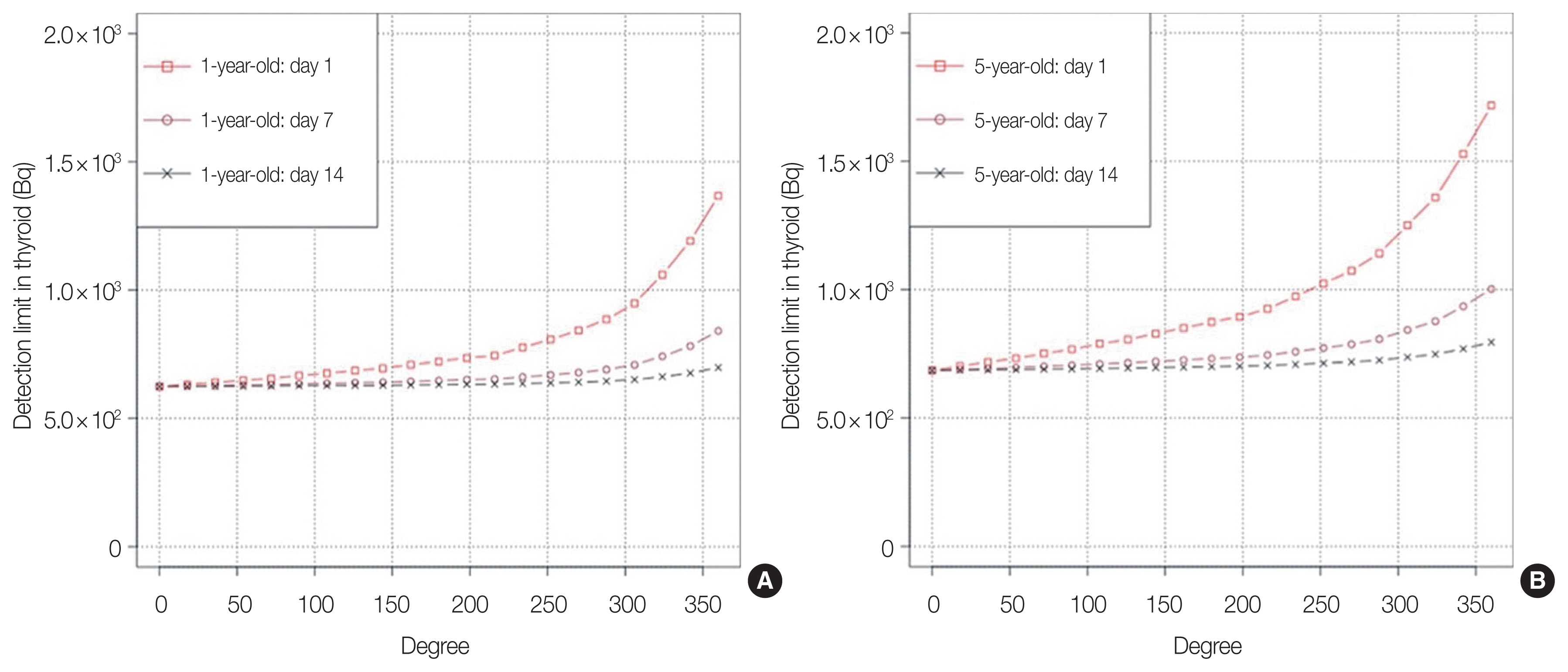
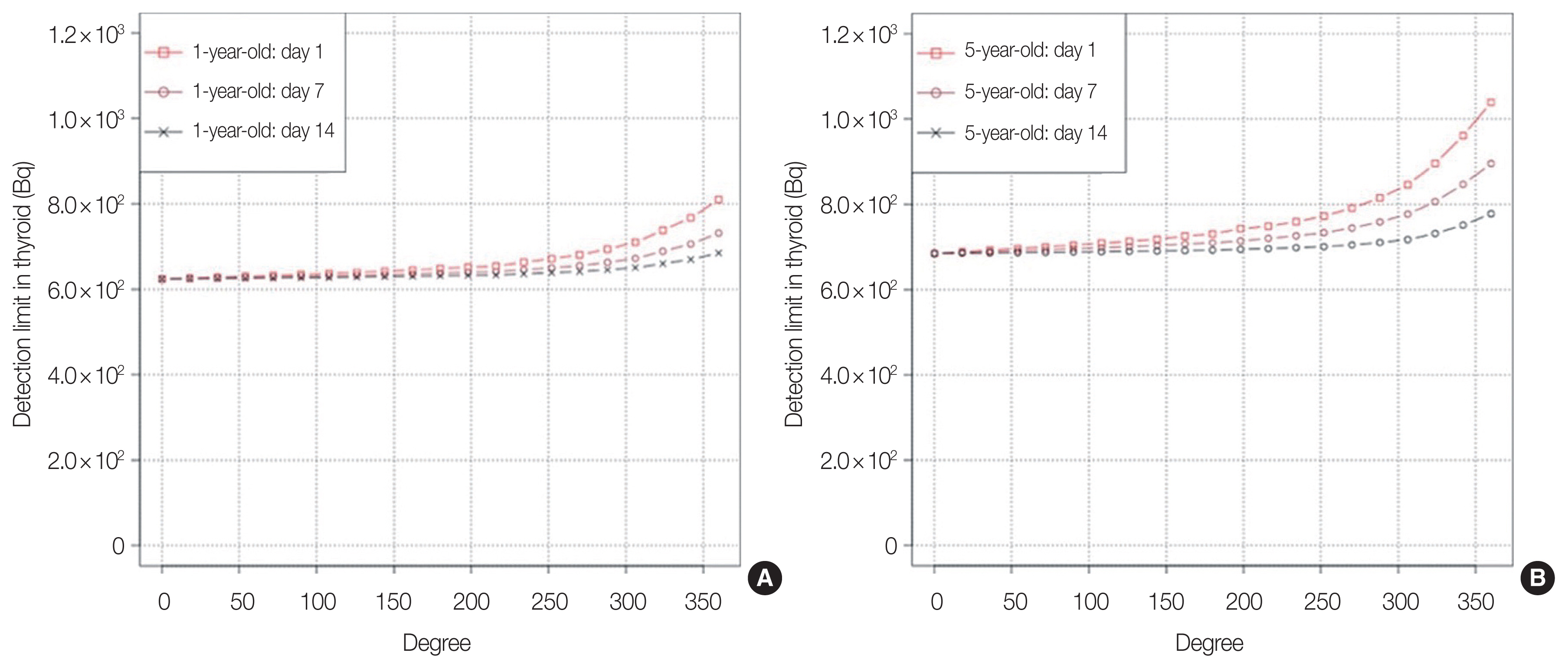
The following figures show the changes in dose rates on days 1, 7, and 14 for 1- and 5-year-old children whose necks were contaminated with eight radionuclides (40 Bq/cm2) (Fig. 6) and when only 131I contamination was spread (Fig. 7). The cervical contamination range extended from the back of the neck (0°) around the entire neck (360°) in 18° increments. When all eight nuclides contaminated the body surface, early measurements showed a higher effect of the short-lived nuclides 132Te and 132I, indicating that the ratio of contaminating nuclides on the body surface changes with the time of measurement.
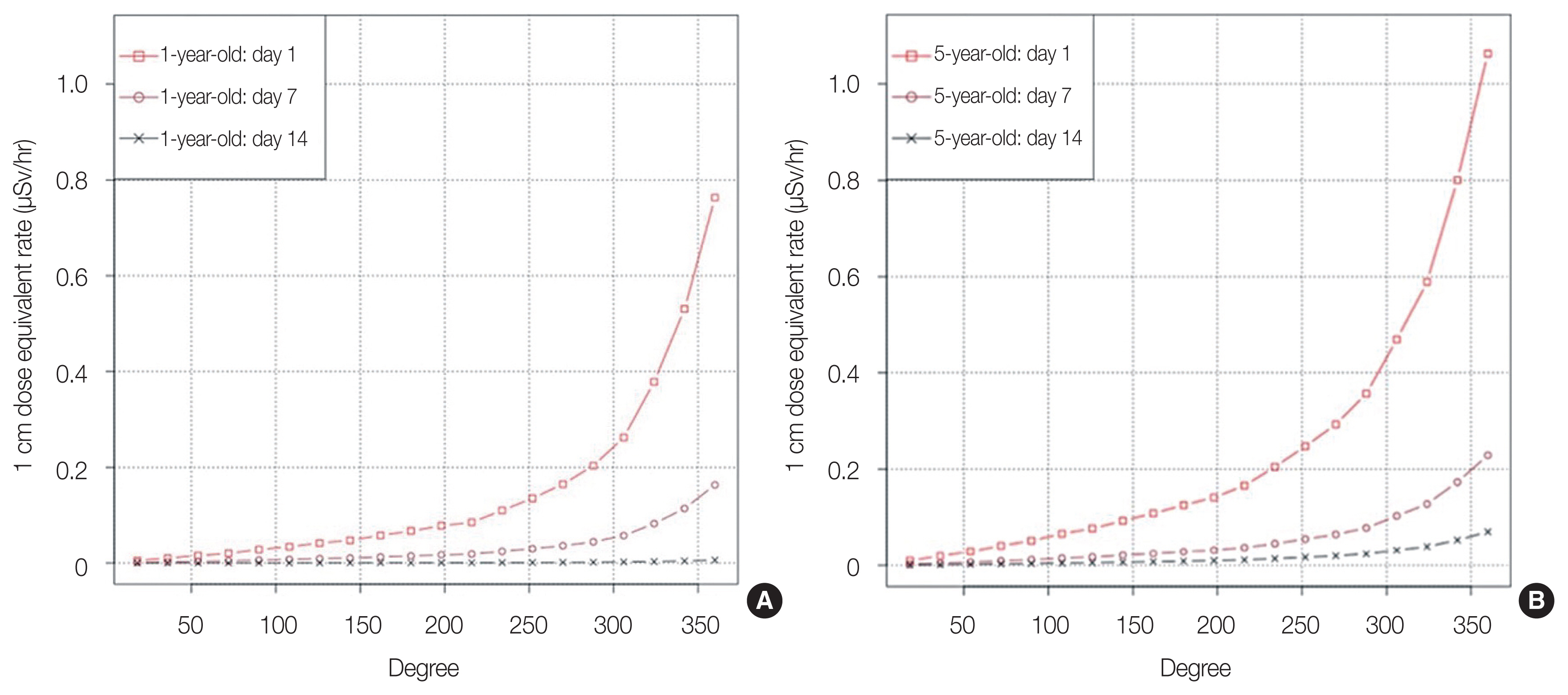
Indicated values (1 cm dose equivalent rate) of NaI(Tl) scintillation survey meter reproduced using the Particle and Heavy Ion Transport code System code for the case of 40 Bq/cm2 contamination of the body surface of the neck by eight nuclides. Comparison of 1-year-old children (A) and 5-year-old children (B) is shown when the range of contamination by radioactive materials on the neck and the time of measurement were varied.
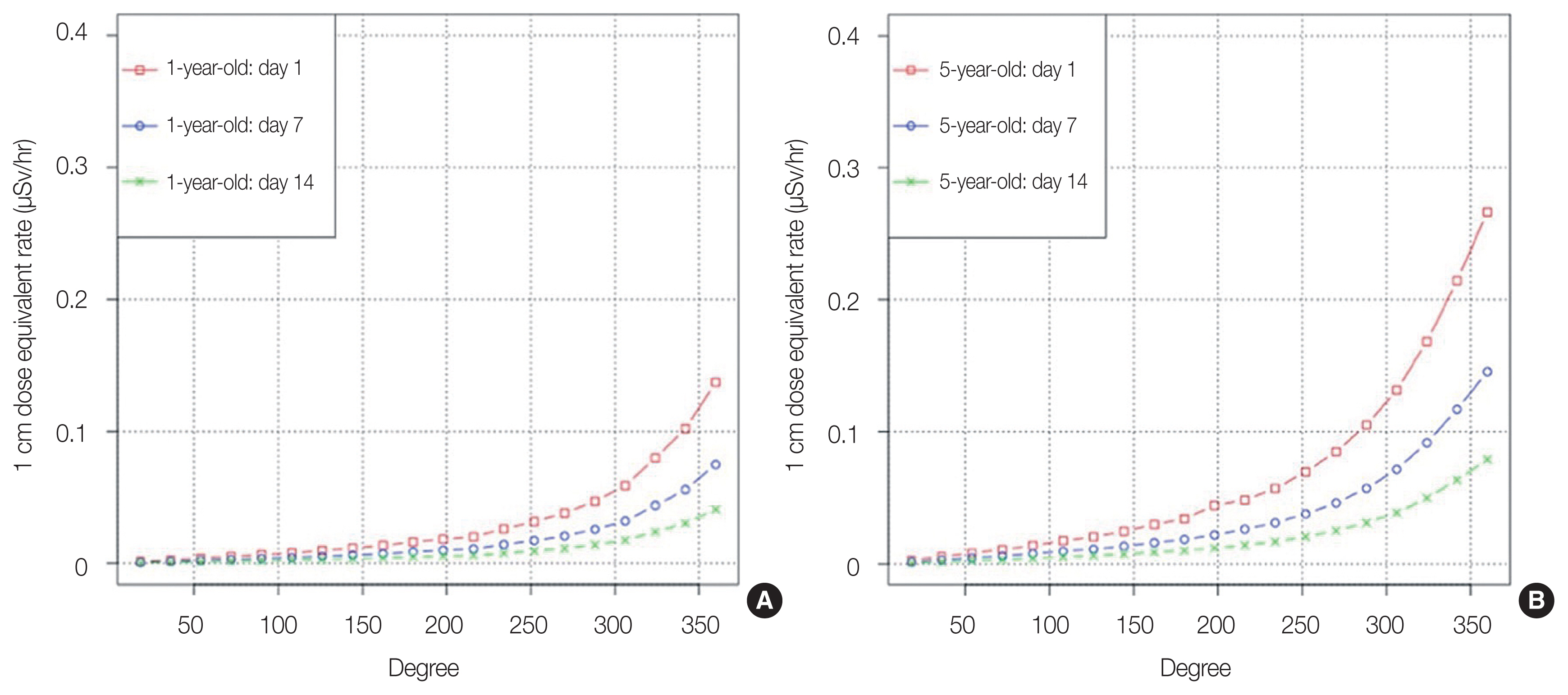
Indicated values (1 cm dose equivalent rate) of the NaI(Tl) scintillation survey meter reproduced using the Particle and Heavy Ion Transport code System code in the case of neck contamination with 131I only. Comparison of 1-year-old children (A) and 5-year-old children (B) is shown when the range of contamination by radioactive materials on the neck and the time of measurement were varied.
3. Detection Limit in the Case of Neck Contamination
In the event of the FDNPP accident, it was reported that simple measurements were conducted by looking for a measurement place with ambient dose rates of 0.2 μSv/hr or lower [4, 5]. Detection limits were determined according to the Equation (3). Calculation of detection limits used threefold standard deviation (3σ) of the output error of the 1 cm dose equivalent rate μSv/hr where the measured dose rate includes the dose rate from contamination of the entire neck at the probe location plus the ambient dose rate. The detection limits were obtained for the case in which the neck was contaminated with eight nuclides (Fig. 8) and the case in which the neck was contaminated only with 131I (Fig. 9) when the time constant of 10 seconds was used. Simple measurements were performed under the exposure scenario in which the ambient dose rate was 0.2 μSv/hr. The simulation was performed by setting the back of the neck at 0° and extending the contamination range to the front of the neck. In comparing 1- and 5-year-old, the effect on the measured values was greater for 5-year-old due to the larger area of the cervical surface. When the timing of the simple measurement was varied from day 0, 7 to day 14, the effect of short-lived nuclides such as 132Te and 132I was significant on day 0, indicating that the ratio of contaminating nuclides on the body surface changes with the measurement timing.
The body surface of the neck was contaminated with 40 Bq/cm2 of eight nuclides, and the detection limit is shown when measured under the conditions of a time constant of 10 seconds and an environmental contribution of 0.2 μSv/hr. Comparison of 1-year-old children (A) and 5-year-old children (B) when the range of contamination by radioactive materials on the neck and the time of measurement were varied.
Detection limits for the case of 40 Bq/cm2 contamination of the neck by 131I only, measured at a time constant of 10 seconds and an environmental contribution of 0.2 μSv/hr. Comparison of 1-year-old children (A) and 5-year-old children (B) when the range of contamination by radioactive materials on the neck and the time of measurement were varied.
Detection limits are shown for the case of 360° contamination with eight nuclides (Fig. 10) and the case of contamination with 131I only (Fig. 11) in a situation in which radioactive materials adhered to the neck only, chest only, and neck+ chest. Detection limits for both the neck and chest were determined by fixing the case of 360° of contamination. The effect on measured values was greater for neck contamination than for chest contamination. As the dose coefficient from 131I differs between 1- and 5-year-old children, the detection limit should be calculated according to the age of the child. The calculations shown here are based on the assumption that 100 mSv of thyroid equivalent dose, corresponding to approximately 7,000 Bq for 1-year-old children and approximately 12,000 Bq for 5-year-old children, accumulates in the thyroid glands of 1-year-old children and 5-year-old children, respectively. The radioactivity of 131I accumulated in the thyroid gland was calculated as the radioactivity of 131I that gave a thyroid dose of 100 mSv using the dose coefficient listed in ICRP Publication 56 [20].
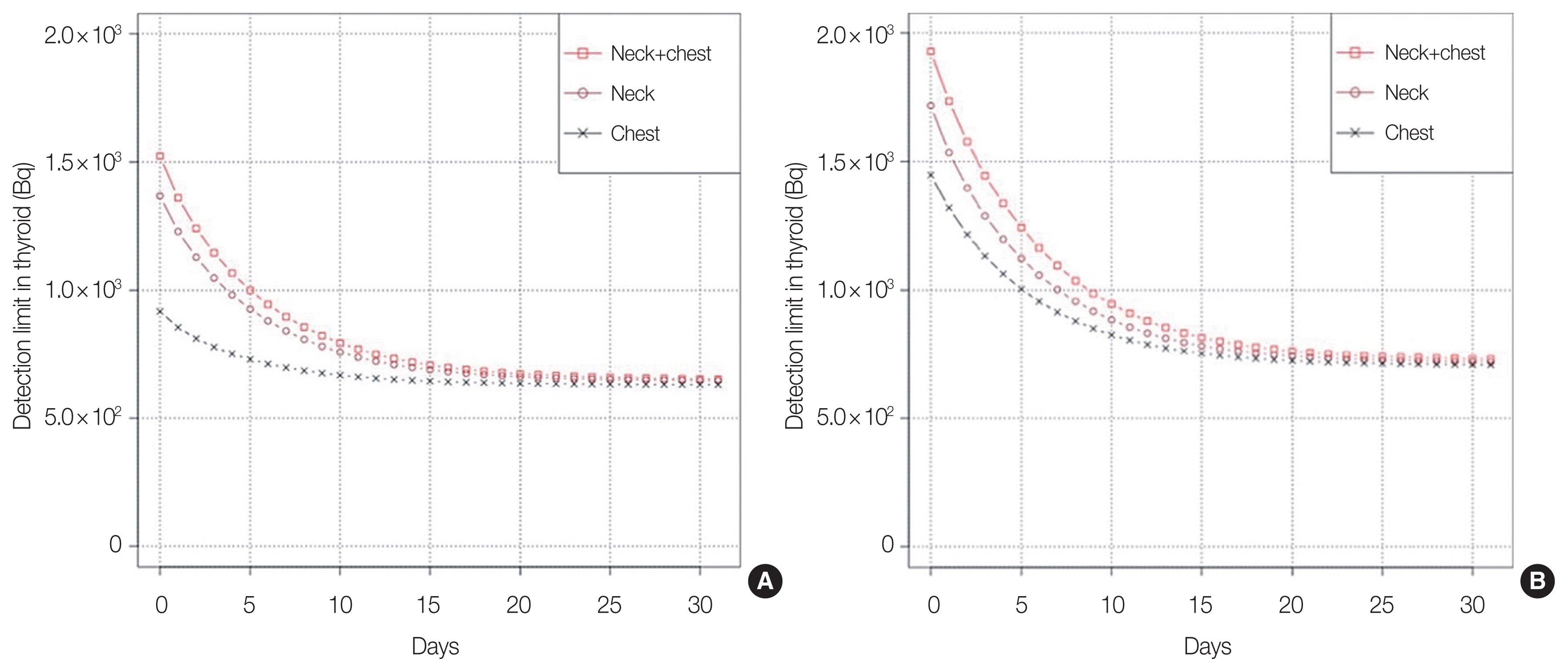
The body surface of the neck was contaminated with 40 Bq/cm2 of eight nuclides, and the detection limit is shown when measured under the conditions of a time constant of 10 seconds and an environmental contribution of 0.2 μSv/hr. The measurement time was varied to compare 1-year-old children (A) and 5-year-old children (B) when the neck was contaminated in 360°, when the shoulder was contaminated, and when both the neck and the shoulder were contaminated.
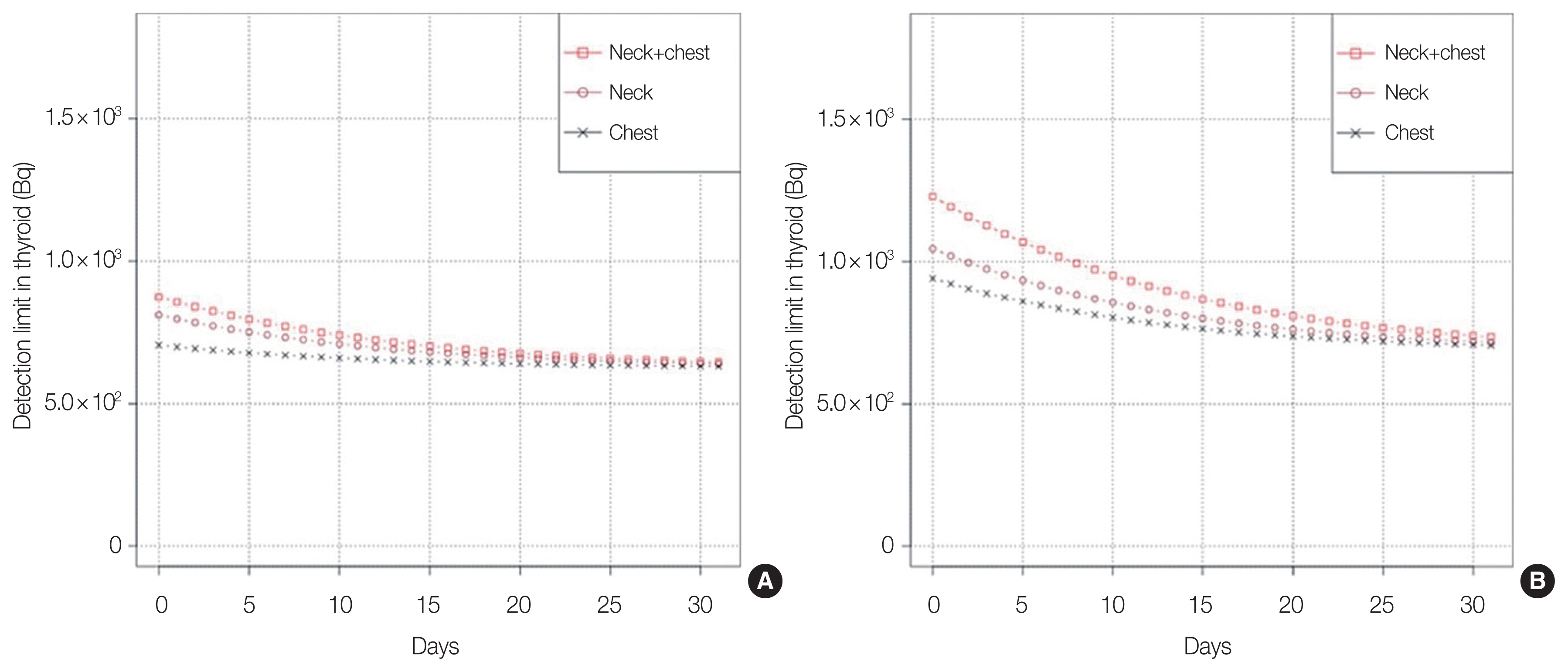
The body surface of the neck was contaminated with 40 Bq/cm2 of 131I alone, which is the detection limit when measured at a time constant of 10 seconds and an environmental contribution of 0.2 μSv/hr. The measurement time was varied to compare 1-year-old children (A) and 5-year-old children (B) when the neck was contaminated in 360°, when the shoulder was contaminated, and when both the neck and shoulder were contaminated.
4. Effects of Ambient Dose Rates on the Detection Limits
For the ambient dose rates from 0.2, 1.0, and 2.0 μSv/hr, Fig. 12 shows the detection limits for 1- and 5-year-old children under fixed conditions of contamination of the cervical body surface with eight nuclides at 360°, when the depth of the thyroid gland is 3 cm. It shows the residual thyroid radioactivity after a single intake of 131I and the detection limits as a function of ambient dose rate. After the FDNPP accident, simple measurements were taken from 12 to 18 days after the accident. Assuming an ambient dose of 0.2 μSv/hr, it was confirmed that thyroid equivalent doses of 100 mSv could be detected for approximately 3 weeks for a 1-year-old child and approximately 1 month for a 5-year-old child.
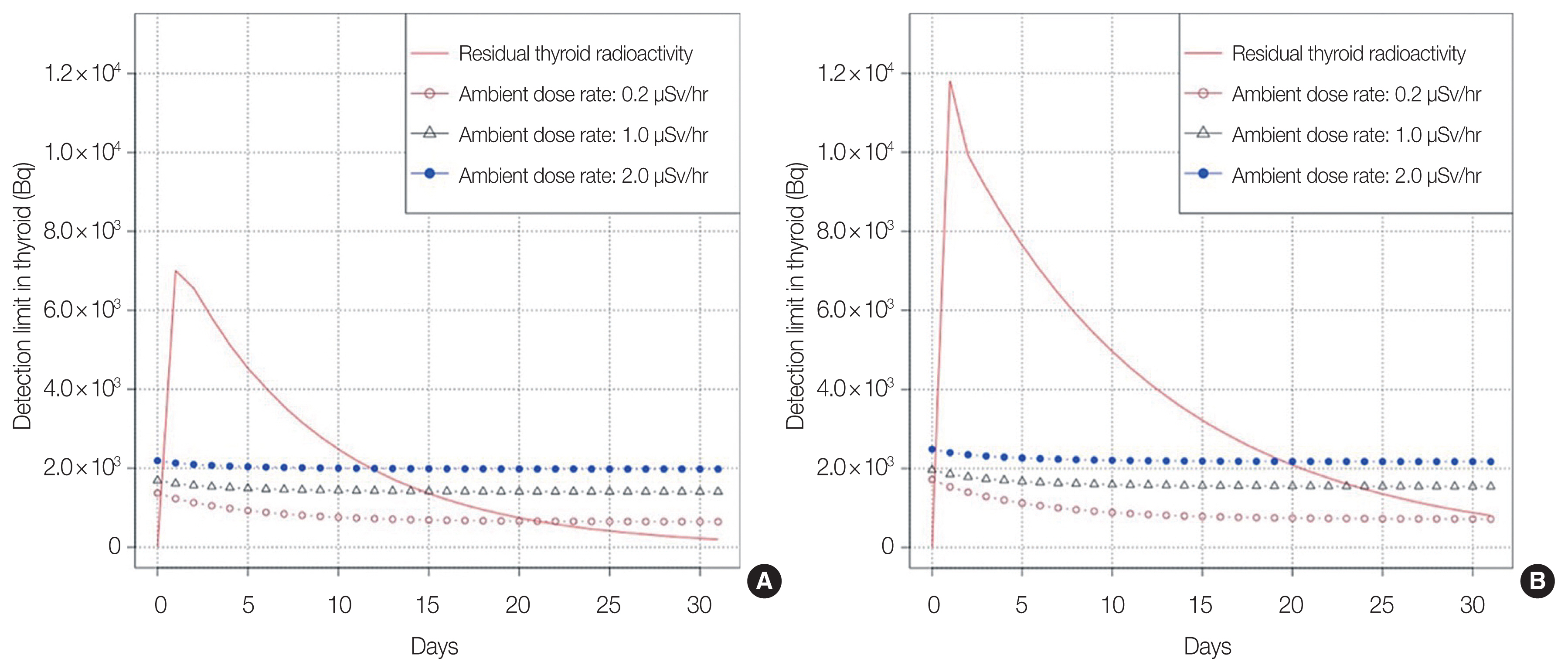
The body surface of the neck was contaminated with 40 Bq/cm2 of eight nuclides, which is the detection limit for a 360° contamination of the neck. The time constant was set to 10 seconds, and the dose rate and timing of the measurements were compared between 1-year-old children (A) and 5-year-old children (B) when the time constant was set to 10 seconds and the dose rate and timing of the measurements were varied. Fig. 12 shows the residual thyroid radio-activity after a single intake of 131I and the detection limits as a function of ambient dose rate.
5. General Consideration of Thyroid Measurement
When performing thyroid measurements on affected children, it is desirable to measure 131I as soon as possible after a nuclear accident because of its short half-life of 8 days. However, immediately after the accident, radioactive materials with a shorter half-life adhere to body surfaces and ground surfaces, so the effect on measurements is larger. According to the results of actual measurements at the FDNPP accident, the net 1 cm dose equivalent rate from the thyroid gland was approximately 0.01 to 0.07 μSv/hr [19]. Residual radioactivity in the thyroid gland can be strongly influenced by ambient dose rates and radioactive materials adhering to the body surface, making it very difficult to selectively measure dose rates from the thyroid gland.
An unavoidable aspect of actual measurements is the effect on measured values due to radioactive materials adhering to the body surface (i.e., skin) of the neck. When detecting 131I accumulated in the thyroid gland, it is appropriate to install a collimator on the survey meter to reduce the influence of an ambient radiation. In this study, however, simulations were conducted assuming that no collimators were installed, because the simple measurements conducted at the time of the FDNPP accident were not equipped with collimators.
Fig. 10 shows the results of measurements of the body surfaces of the neck, chest, and neck+chest contaminated with eight nuclides, and Fig. 11 shows the results of measurements of the body surfaces of the neck, chest, and neck+chest contaminated only with 131I. As the skin of the neck is inevitably directly contaminated with radioactive materials, the measurement will be affected if the skin surface is not sufficiently decontaminated.
6. Effects of Cervical and Shoulder/Chest Contamination
As children are often carried by their parents during an evacuation, we assumed that contamination would spread from the back of the neck. Contamination of the shoulder area assumes that the collar has been contaminated; the FDNPP accident occurred in March, and people were thought to have evacuated wearing warm clothes at that time. The effect on the measured values due to radioactive materials adhering to clothing was not assessed in this investigation because it can be avoided by removing the clothing. Comparing the neck and shoulders, Fig. 6 shows that the effect of radioactive materials on both the neck and shoulders was larger in 5-year-old children than in 1-year-old children because of the larger area of contamination on the body surface in the older children. However, Fig. 8 shows that the detection limit was lower for 1-year-old children. The reason for this difference is that the amount of 131I that accumulates in the thyroid gland, which is equivalent to a thyroid dose of 100 mSv, differed between 1-year-old children and 5-year-old children because of differences in the biokinetics of 131I and thyroid mass. This study revealed that the detection limit became more stringent as the degree of radioactive contamination on the body surface and that the detection limit varied by age.
7. Effects of Short-Lived Nuclides
The presence of short-half-life radioactive materials on the body surface affects the detection limit. The ratio of radioactive materials changes over time because short-lived radioactive materials adhering to the body surface decay with different half-lives. The ratios of radioactive materials used for this investigation were matched to the ratios of radioactive materials measured on the clothing of evacuees during the FDNPP accident. The ratios were determined by scans using a whole-body counter equipped with a Ge γ-ray spectrometer. Short- and long-lived radionuclides found on clothing included 131I, 132I, 132Te, 133I, 135I, 134Cs, 136Cs, and 137Cs. After correcting for physical decay as of 12:00 PM on March 12, the radioactivity ratios were assumed to be 132Te(132I):133I:135I:134Cs:136Cs: 137Cs:131I as 2.3:1.1:0.3:0.1:0.02:0.1:1, and these ratios were used in the investigation [11–13]. In the simulation of the PHITS code, the contribution of the newly produced 132I is included in the 132Te contribution in the calculation. However, since the contribution of 132I that was already attached to the clothing was not included, the calculations were performed based on consideration of physical attenuation due to the half-life of 132I. The effect on the measured values of short-lived nuclides adhering to the body surface is expected to be small for estimating residual thyroid radioactivity in the case of body surface contamination of approximately 40 Bq/cm2, but the effect on the measured values is expected to be high when the body surface contamination density is high or the percentage of nuclides with high γ-ray emission rates is high. In the case of the present ratios, the highest impact was observed for 132Te and its descendant nuclide 132I.
8. Effects of Short-Lived Nuclides on Thyroid Doses
The present calculation assumes exposure to body surface contamination that could result in intake of 131I equivalent to 100 mSv of thyroid equivalent dose. Iodine is necessary for the synthesis of thyroid hormones, and orally ingested iodine is readily absorbed from the gastrointestinal tract. After entering the bloodstream, 30% accumulates in the thyroid gland, 10% is rapidly excreted, and the remainder is excreted from the body in a short time. The disappearance rate from the thyroid gland is age-dependent, with a biological half-life of 20 days in 1-year-old children, 30 days in 5-year-old children, and 91 days in adults [20]. The dose coefficients for each age group described in ICRP Publication 71 were used to determine the intake amount, and the thyroid deposition rate of 131I was determined using the MONDAL system database published by the Quantum Science and Technology Development Institute of Japan [21, 22]. The thyroid deposition rate of 131I is calculated by multiplying the intake by the deposition rate. Exposure to beta radiation significantly affects the equivalent dose to the thyroid gland. In the event of the FDNPP accident, 131I represented only 20% of the total radioactivity of the eight nuclides adhering to the body surface of evacuees. Other radionuclides include 132I, 132Te, and 133I. The dose coefficient can be thought of as the equivalent dose (Sv) per organ per (Bq), and the dose coefficient for 131I is 3.2× 10−6 Sv/Bq for a 1-year-old child, making 131I the highest of the three nuclides [20]. Based on the above results, 131I among radioiodine isotopes has the largest effect on the thyroid gland, and this study using similar methods for various other nuclides showed that 132I and 133I are difficult to detect after the passage of approximately 1 and 5 days, respectively, between release and measurement. In this study, thyroid doses were estimated only for 131I, but it is also desirable to estimate doses considering the effects of short-lived nuclides such as 132I and 133I.
In the case of ambient dose rates of 1.0 and 2.0 μSv/hr, it was confirmed that measurement of a thyroid equivalent dose of 100 mSv was possible up to days 14 and 11 for 1-year-old children and up to days 20 and 17 for 5-year-old children, respectively. However, 131I activity in thyroids peaks between 1 and 2 days after intake and decays by its effective half-life. Considering the effective half-life of 131I, it is required to measure the thyroid activity as early as possible, but it is desirable to measure it 2 days after intake because measurement immediately after intake would result in underestimation.
It is desirable to measure the state of contamination of the neck surface using a GM tube survey meter capable of measuring β-rays in order to confirm that there is no surface contamination. If there is high surface contamination of the neck area, it is necessary to decontaminate the area and confirm that contamination has been reduced to a level that will not affect simple measurements. After the FDNPP accident, the time constant was set to 10 seconds, and the average of three readings of the indicated value after 30 seconds from the start of the measurement was recorded. As a result, the effect of reading error was estimated to have been smaller than that in the present study. In actual measurements, it is recommended that the average of three readings should be used to minimize reading errors.
9. Effects of Thyroid Depth and Height Due to Differences in Body Shape
Because the depth of the thyroid gland in children varies greatly depending on their body shape, Table 2 shows a simulation in which the depth and height of the thyroid gland were varied in the case of an accumulation of approximately 7,000 Bq of 131I in the thyroid gland, which is considered equal to a thyroid dose of 100 mSv. A depth of thyroid in Table 2 shows the case in which depth was varied. Comparing 2.0 and 3.0 cm, there was a difference of approximately 43%. A height of thyroid in Table 2 shows the case in which the height of the thyroid gland was varied, and a change of ±1.0 cm resulted in a difference of approximately 6.6%, indicating that differences in the position of the thyroid gland have a significant effect on measured values. In particular, depth differences have a higher impact on detection limits, and the inverse square law of distance and absorption by cervical body thickness can significantly affect the indicated value. As classification by age tends to produce differences due to body shape, it is thought that classification by neck size will reduce errors.
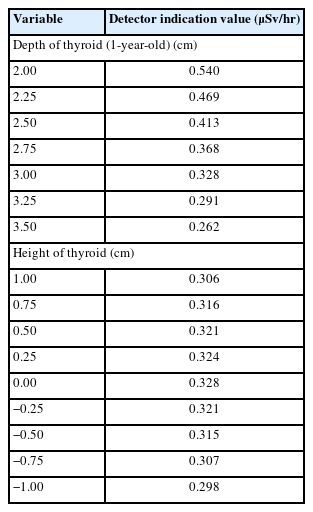
Effects of the Thyroid Locations on Measured Values in Children Aged 1
Conclusion
This study clarified the effect of radioactive materials adhering to body surfaces (neck and chest) on the results of simple measurements using a NaI(Tl) scintillation survey meter by simulations using PHITS. In the absence of the body surface contamination, the detection limit depends only on the ambient dose rate at the measurement location. The results of this study showed that a residual thyroid radioactivity of 600 to 700 Bq can be detected in a 1-year-old child (thyroid gland depth of 3 cm). In the case of 40 Bq/cm2 contamination on the body surface of the neck, the present simulations showed that residual thyroid radioactivity corresponding to thyroid dose of 100 mSv can be detected within 21 days after intake at the ambient dose rate of 0.2 μSv/hr and within 11 days in the case of 2.0 μSv/hr.
Notes
Conflict of Interest
No potential conflict of interest relevant to this article was reported.
Ethical Statement
This article does not contain any studies with human participants or animals performed by any of the authors.
Author Contribution
Conceptualization: Kai M. Methodology: all authors. Data curation: Kitajima T. Formal analysis: Kitajima T. Supervision: Kai M. Visualization: Kitajima T. Software: Kitajima T. Writing - original draft: Kitajima T. Writing - review & editing: Kai M. Approval of final manuscript: all authors.
Acknowledgements
We would like to thank Dr. Kamei, Nippon Bunri University and those who are in Nippon Bunri University Medical College for their valuable discussions and advice.
References
 . Report of the Study Team Meeting on Emergency Thyroid Exposure Dose Monitoring] [Internet]. Nuclear Regulation Authority; 2021. [cited 2023 Aug 25]. Available from: https://www.nra.go.jp/data/000360345.pdf (Japanese).
. Report of the Study Team Meeting on Emergency Thyroid Exposure Dose Monitoring] [Internet]. Nuclear Regulation Authority; 2021. [cited 2023 Aug 25]. Available from: https://www.nra.go.jp/data/000360345.pdf (Japanese).