The Japan Health Physics Society Guideline on Dose Monitoring for the Lens of the Eye
Article information
 , Norio Tsujimura2, Makoto Hashimoto3, Hiroshi Yoshitomi4, Masahiro Kato5, Tadahiro Kurosawa5, Hideo Tatsuzaki6, Hiroshi Sekiguchi7, Yasuhiro Koguchi8, Koji Ono9, Masahumi Akiyoshi10, Naoki Kunugita11, Masahiro Natsuhori12, Yoshinori Natsume13, Kuniaki Nabatame14, Tsunenori Kawashima15, Shunji Takagi16, Kazuko Ohno17, Satoshi Iwai18
, Norio Tsujimura2, Makoto Hashimoto3, Hiroshi Yoshitomi4, Masahiro Kato5, Tadahiro Kurosawa5, Hideo Tatsuzaki6, Hiroshi Sekiguchi7, Yasuhiro Koguchi8, Koji Ono9, Masahumi Akiyoshi10, Naoki Kunugita11, Masahiro Natsuhori12, Yoshinori Natsume13, Kuniaki Nabatame14, Tsunenori Kawashima15, Shunji Takagi16, Kazuko Ohno17, Satoshi Iwai18
Abstract
Background
In Japan, new regulations that revise the dose limit for the lens of the eye (hereafter the lens), operational quantities, and measurement positions for the lens dose were enforced in April 2021. Based on the international safety standards, national guidelines, the results of the Radiation Safety Research Promotion Fund of the Nuclear Regulation Authority, and other studies, the Working Group of Radiation Protection Standardization Committee, the Japan Health Physics Society (JHPS) developed a guideline for radiation dose monitoring for the lens.
Materials and Methods
The Working Group of the JHPS discussed the criteria of non-uniform exposure and the management criteria set not to exceed the dose limit for the lens.
Results and Discussion
In July 2020, the JHPS guideline was published. The guideline consists of three parts: main text, explanations, and 26 examples. In the questions, the corresponding answers were prepared, and specific examples were provided to enable similar cases to be addressed.
Conclusion
With the development of the guideline on radiation dose monitoring of the lens, radiation managers and workers will be able to smoothly comply with revised regulations and optimize radiation protection.
Introduction
From July 2017 to February 2018, the subcommittee of radiation protection of the lens of the eye (hereafter the lens) of the Radiation Council of Japan discussed the implementation of the International Commission on Radiological Protection (ICRP) new dose limit to the lens [1] in the context of Japanese regulations related to radiation protection for radiation workers, and published the subcommittee report [2]. The Council judged it appropriate to revise current Japanese regulations, as recommended in the ICRP Statement on Tissue Reactions. In particular, the equivalent dose limit of the lens should be 20 mSv/yr, averaged over defined periods of 5 years, with no single year exceeding 50 mSv [1]. The Council also recommended revision of the regulations such that the personal dose equivalent at 3 mm depth, Hp(3), can be monitored to estimate the equivalent dose to the lens more accurately; however, it is not mandatory to measure Hp(3) if the equivalent dose of the lens can be adequately estimated using the personal dose equivalent at a depth of 1 cm, Hp(10), or 70 μm, Hp(0.07). In addition, there are various exposure fields, such as the medical sector; therefore, it was expected that related institutions would prepare guidelines or manuals. The Council recommended taking the necessary measures for the related regulations with reference to the subcommittee report.
In December 2018, the Ministry of Health, Labour and Welfare (MHLW) in Japan, which is responsible for the regulations related to occupational health, discussed the implementation of the dose limit and monitoring of the lens as recommended by the Council [3]. The MHLW generally adopted the policy of the Council; however, it provided an interim measure for some clinicians working in radiation facilities who are likely to receive an equivalent dose >100 mSv over 5 years to the eye lenses, even with appropriate radiation protection measures including shielding, and for those who provide medical services that require advanced professional knowledge and experience that cannot be easily substituted. Finally, the MHLW determined that the lens dose limit for these clinicians to be 60 mSv over 3 years and 50 mSv/yr until March 2023 in the Supplementary Provisions of the Amended Regulation. Beginning in April 2023, the lens dose limit will be the same as that for other radiation workers [4–6]. All related regulations submitted by the relevant government agencies were reviewed by the Council until July 2020 [6]. The Council reported that all revised regulations properly reflected their recommendation; however, they commented to a government agency on the thoroughness of dosimetry and reports of doses to decommissioning workers [7]. All-related regulations were enforced in April 2021. The equivalent dose limit to the lens was revised from 150 mSv/yr to 100 mSv over 5 years and 50 mSv/yr. The personal dose equivalent, Hp(3), will be added to the current operational quantities for lens dose monitoring, the personal dose equivalents, Hp(10) and Hp(0.07). The measurement regions and operational quantities under the previous regulations and revisions are shown in Fig. 1.

Dose measurement regions and operational quantities under Japanese regulations.
The development of radiation protection applications for the new dose limit to the lens was supported by the Radiation Safety Research Promotion Fund of the Nuclear Regulation Authority (NRA), Japan [8–10]. In 2019, we began to prepare a guideline on radiation monitoring for the lens related to all fields and radiation protection in the medical sector in cooperation with related academic societies under the NRA fund [10]. The Working Group of the Radiation Protection Standardization Committee, the Japan Health Physics Society (JHPS) [11], discussed the guideline on radiation monitoring for the lens while referring to the research of the NRA fund. In July 2020, the JHPS guideline on radiation monitoring for the lens was published in Japanese [12].
The Working Group of the JHPS Radiation Protection Standardization Committee consisted of researchers involved with radiation protection and dosimetry in the medical and nuclear fields, representatives of radiation managers from nuclear power plants, technical experts of dose monitoring, and observers such as radiation managers from nuclear power plants and technical experts in nuclear industries. The Committee discussed the draft guideline and invited the opinions of the society members. Some comments were reflected in the draft guideline. Finally, the guideline was published with the approval of the JHPS Board of Directors.
Basic Concept of the Guideline on Radiation Dose Monitoring for the Lens of the Eye
1. Basic Concept
The guideline consists of three parts: Main text, Explanation, and Examples (questions and answers). The Explanation contains three documents related to the current national and international status of the dose limit of the lens, the International Atomic Energy Agency (IAEA) proposal for monitoring the equivalent dose to the lens [13], and previous monitoring methods of the equivalent dose to the lens [14].
In particular, the following points were noted while developing the guidelines: (1) compliance with the revised regulations for dose monitoring of the lens, (2) harmonization with the existing monitoring methods for measuring the effective and equivalent dose to the skin, (3) optimization of dose monitoring and radiation protection in radiation workplaces and situations, and general occupational safety and health; (4) supporting radiation managers by providing a simple and easy-to-understand concept for radiation monitoring of the lens, including scientific evidence; and (5) advice on the judgment of criteria of non-uniform exposure and dose management criteria for the lens to be decided by each radiation facility.
2. Highlights of the Lens Dose Monitoring
Main text consists of two chapters: scope of application and guidance on dose monitoring. In Chapter 1, the monitoring points, exposure situation and type of radiation are specified. In Chapter 2, we describe the region for dose monitoring under uniform and non-uniform trunk exposure situations, and the operational quantities used for monitoring.
1) Scope of application
In Chapter 1 of Main text, the scope of application has been illustrated as follows: the guideline is to be applied to monitor the lens for radiation workers under planned exposure situations and exposure to photons, electrons (>700 keV), and neutrons. This approach was taken because alpha particles and electrons (<700 keV) cannot reach the radiation-sensitive part of the lens [1, 13]. Section 5(2) of Explanation of the guideline describes the reasons for applying these radiation types and situations.
2) Guidance on dose monitoring
It is shown in Chapter 2 of Main text that dose monitoring regions and the operational quantities for the lens are determined by two steps. In the first step, the dose monitoring methods for the lens should be discriminated into two patterns depending on the uniform exposure. Details on the uniform or non-uniform exposure situations have been explained in detail in Section 5(5) of Explanation. In the second step, monitoring methods are decided by whether the dose to the lens was close to or exceeded the management criteria for each type of exposure (uniform or non-uniform trunk exposures). The management criteria should be set to conservative values below the dose limits and decided by the employer or radiation dose manager in each facility. However, it may be challenging to determine the values of the criteria; thus, references and numerical values have been shown in Explanation (Section 5(3)) and Examples (Example 3). Fig. 2 illustrates the dose monitoring for the lens to aid understanding.
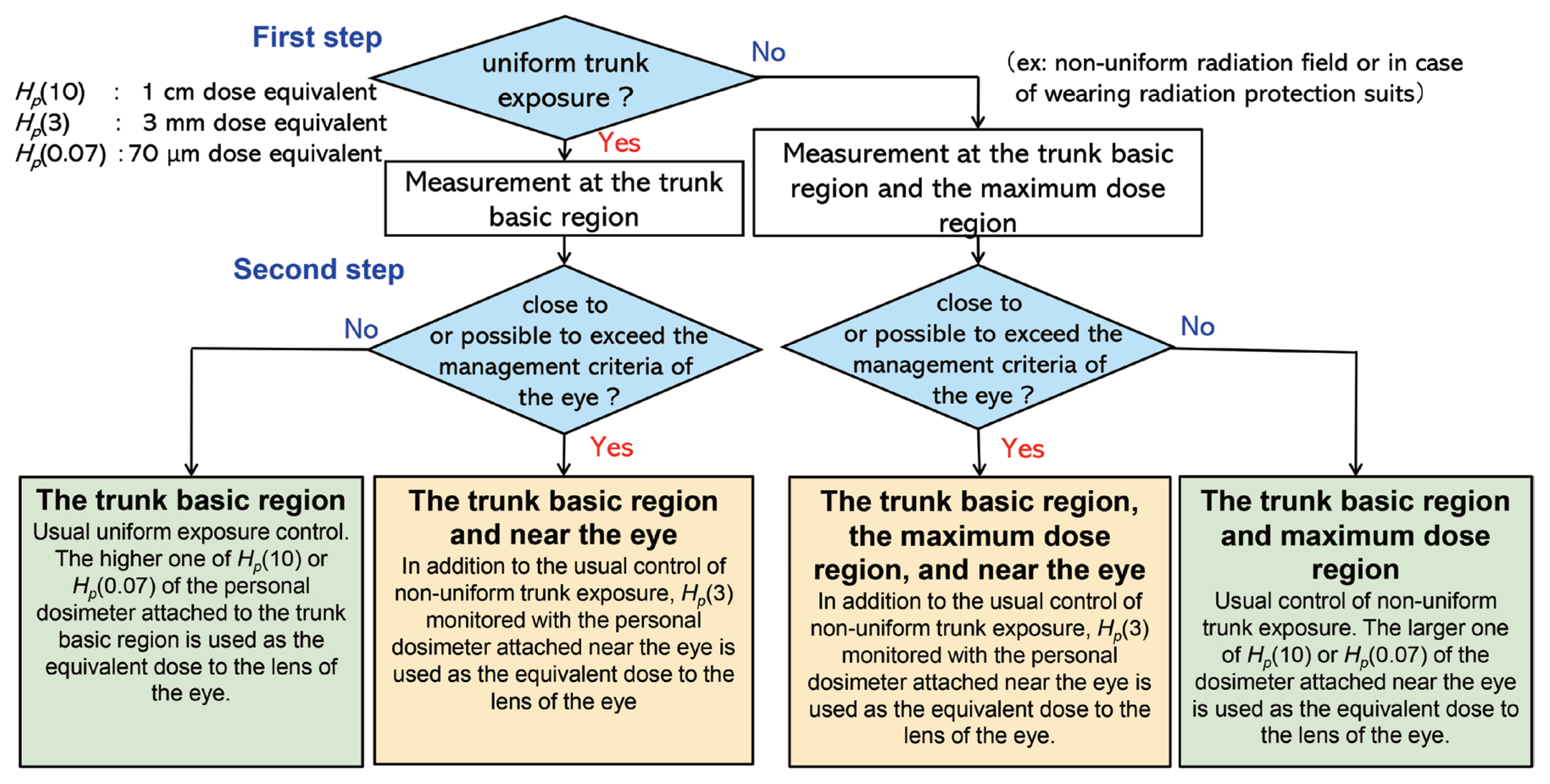
Flow diagram for lens dose monitoring.
3. Detailed Explanation of the Lens Dose Monitoring
1) Explanation outline
The Explanation consists of five chapters: (1) Objective, (2) Scope of application, (3) Related acts and regulations, (4) Glossary, and (5) Monitoring methods to estimate the dose equivalent of the lens. In addition, it includes the three documents mentioned in 1. Basic concept.
2) Objective
The “Measurement and estimation manual of the exposed dose” [14] was prepared when the related regulations were revised based on the ICRP Publication 60 [15]. This is a comprehensive manual that includes a method to estimate the effective doses for internal and external exposures and provides the equivalent doses for external exposure that have been used by Japanese radiation workers. The revised regulations did not change the effective dose limit, the equivalent dose limit to the skin, and the related dose estimation methods; however, the dose limit to the lens was revised and the operational quantities and measurement area for estimation of the lens dose were added. This guideline only covers lens dose monitoring, and “Measurement and estimation manual of the exposed dose” must continue to be used for other aspects. Thus, this guideline supplements the lens dose monitoring part of “Measurement and estimation manual of the exposed dose” in the Objective.
3) Scope of application
Chapter 2 of Explanation elucidates the application of the guideline on the individual dose monitoring of radiation workers under the planned exposure situation of workplaces described in ICRP Publication 103 [16]. Radiation monitoring under emergency and existing exposure situations has not been included in the scope of application of the guidelines. However, the basic concept of dose measurement for the lens would be helpful in these exposure situations.
4) Monitoring methods to estimate the lens dose equivalent
Chapter 5 of Explanation consists of the following seven sections: (1) basic concepts, (2) type of radiation applied, (3) desirable dose level of monitoring directly near the eye (management criteria), (4) recording the equivalent dose to the lens of the eye, (5) monitoring regions to estimate the equivalent dose to the lens of the eye, (6) operational quantity used to estimate equivalent dose to the lens, and (7) the methodology used to judge whether the equivalent dose to the lens of the eye is close to or may exceed the management criteria.
In particular, the judgment of the exposure situations (uniform exposure or not) and the management criteria for the lens dose monitoring are discussed in Sections (3) and (5) of Explanation Chapter 5.
4. Specific Examples
Twenty-six related questions along with their answers have been included to guide responses in similar cases, such as the judgment and management criteria for the exposure situations, optimization of the radiation protection for the lens, available personal dosimeters for the lens, calibration methods for the personal dosimeters for the lens, national current status of radiation exposure for the lens in medical and nuclear fields, international and national guidelines for dosimetry, dose estimation methods for electrons, indirect estimation by calculation, and more. Table 1 presents a list of these questions.

List of the Questions
The Examples were selected and developed by engaging the opinions of the Working Group members, especially the radiation managers familiar with radiation and nuclear workplaces. The answers were prepared for experts in each field. Reference dose levels for judging the exposure situations and direct measurement near the eye have been provided in Examples 1 and 3, respectively.
The response to Example 4 regarding the possibility of lens dose estimation by monitoring with a personal dosimeter attached to the outside of the full-face mask and by the calculation using a shielding factor has been drafted by referring to the MHLW report [3]. The MHLW report stated that it is appropriate to measure personal dosimeters inside the full-face mask when personal protective equipment is worn. In contrast, paragraph 3, Article 8 of the Regulation on Prevention of Ionizing Radiation Hazards [5] states, “when it is very difficult to measure the dose using a radiation measuring instrument, the dose can be estimated by calculation.” Here, “very difficult to measure the dose” indicates a situation in which radiation dosimeters have not yet been developed [17]. Therefore, for such a case, the example was shown that it would be appropriate to use personal dosimeters inside the full-face mask directly.
Discussion
1. Judging the Exposure Situations
The revised regulations would make the judgment of the exposure situations challenging because the value of the equivalent dose limit to the lens is equal to that of the effective dose limit. The manual, “Measurement and estimation manual of the exposed dose”, recommended wearing an additional dosimeter when the maximum dose was more than three times the dose measured in the basic trunk region, chest, or waist [14]. This concept was based on the ratio of the previous lens dose limit to the effective dose limit (150 mSv/50 mSv=3). However, this ratio cannot be used under the new regulations. Therefore, ICRP Publication 75 [18], IAEA GSG-7 [19], and expert advice on previous regulations based on the ICRP 1977 recommendation [20] were referenced. In the ICRP Publication 75 [18] and the IAEA GSG-7 [19], the range of the uncertainties of 1.5 to 2 in personal monitoring was helpful to consider this indicator, although indicators of non-uniform exposure situation have not been recommended. Alternatively, radiation experts recommended that multiple personal dosimeters be attached when the dose ratio is only 2 [20]. Thus, it was concluded that the judgment criteria of the exposure situations were 1.5 to 2 in this guideline. These criteria have been explained in detail in Explanation, and a specific description has been added to Example 1.
2. Management Criteria
The management criteria should be set to conservative values below the dose limits and decided by the employer or radiation dose manager in each facility, as mentioned above. However, the guideline must provide the concept and reference examples for the management criteria of the lens dose monitoring.
The concept of individual monitoring was based on ICRP Publication 75 [18]. In addition, the “Measurement and estimation manual of the exposed dose” [14] supported the discussion of the criteria. These criteria are associated with measurement uncertainty and non-uniform exposure. Example 3 gives a specific example that it may be better to wear a personal dosimeter near the lens of the eyes. Given the general uncertainty of a factor of 1.5 in personal dosimeter measurements, differences in readings of two dosimeters exceeding a factor of 1.5 are regarded as significant. Therefore, when the annual dose equivalent, Hp(10) or Hp(0.07), measured by the personal dosimeter attached in the basic trunk or the maximum dose region is likely to exceed the criteria of 13 mSv (=20 mSv/1.5), additional use of lens dosemeters is recommended. Furthermore, when the job-specific uncertainty can be estimated to be a factor of 1.2 based on the workplace study, an example was also shown that the criteria could be set to 17 mSv/yr (≈20 mSv/1.2). In addition to these values, the applicable management criterion of the direct measurement near the lens indicated in IAEA TECDOC No. 1731 [13], the Council Directive 2013/59/EURATOM [21], the ISO 15382: 2015 [22], the International Radiation Protection Association (IRPA) Guidance [23], and our research supported by the Radiation Safety Research Promotion Fund [9] were proposed as references. The results are shown in Table 2.

Management Criteria to Judge the Direct Measurement near the Eye as References
Conclusion
In the JHPS, the guideline on dose monitoring for the lens was developed by radiation protection experts. The guidelines were based on international standards and guidelines, new and old national regulations, and research results. The important issues regarding the operational quantities and the measurement regions for the dose estimation of the lens were clarified by expert discussions and considerations. Hopefully, the guideline will be effectively used for compliance with the related regulations of dose monitoring and optimization of radiation protection for the lens, including radiation monitoring. However, the guideline should be revised as necessary when new knowledge, technologies, and methods for monitoring will emerge in the future.
Acknowledgements
We would like to thank members of the Japan Health Physics Society (JHPS) Board, the Radiation Protection Standardization Committee of the JHPS, and associate members of the Working Group for their support and valuable comments.
This research was partially supported by the 2019 Radiation Safety Research Promotion Fund, the Nuclear Regulation Authority (No. JPJ007057).
Notes
Conflict of Interest
No potential conflict of interest relevant to this article was reported.
Author Contribution
Project administration: Yokoyama S. Funding acquisition: Yokoyama S. Writing - original draft: Yokoyama S. Writing - review and editing: Tsujimura N, Hashimoto M, Yoshitomi H, Kato H, Kurosawa T, Tatsuzaki H, Sekiguchi H, Koguchi Y, Ono K, Akiyoshi M, Kunugita N, Natsuhori M, Natsume Y, Nabatame K, Kawashima T, Takagi S, Ohno K, Iwai S. All the authors have proofread the final version.